Article Text

Abstract
Purpose A prospective, randomised, masked study comparing three different intraocular infusion solutions used during vitrectomy on postoperative electroretinography (ERG) and retinal histology of rabbit eyes.
Methods, materials and animals Twelve rabbit eyes were used with each group of three intraocular infusion solutions: Lactated Ringers (LR), balanced salt solution (BSS) and balanced salt solution-plus (BSS-Plus).
Results At 24 hours postoperatively, the ERG values were 36%, 68% and 75% of the normal values for LR, BSS and BSS-Plus, respectively. At 72 hours postoperatively, the ERG values were 50%, 84% and 100% of the normal values for LR, BSS and BSS-Plus, respectively. At 72 hours postoperatively, 3/12, 10/12 and 12/12 of the vitrectomised eyes had regained normal-value ERGs for LR, BSS, and BSS-Plus eyes, respectively. At 1 week postoperatively, 4/12 and 12/12 of LR and BSS eyes, respectively, had normal ERGs. The number of LR eyes regaining normal ERG values was 4/12, 6/12 and 9/12, measured at 1, 4 and 15 weeks postoperatively, respectively.
Retina histology At 15 weeks follow-up, histopathology was performed on several rabbit eyes. Histological examination of LR-irrigated eyes showed 2/7 normal retinas, whereas 5/7 showed changes that ranged from vacuoles in the inner retina to numerous vacuoles in both the outer and inner retina with disruption of the inner nuclear layer. The histology of BSS-infused and BSS-Plus-infused rabbit eyes was normal.
Conclusion LR solution, when used during vitrectomy, has a more prolonged negative effect on ERG than BSS and BSS-Plus. Histological changes seen in LR eyes may explain the ERG results.
- Infusion solutions
- Vitrectomy
- Scotopic ERG
- Rabbit
- Retina histology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Although in the past all three solutions have been used for vitrectomy irrigating solutions, they are possibly not comparable in maintaining optimal retinal health during and after retinal surgery. Lactated Ringers appears to be an inadequate substitute for balanced salt solution-plus (BSS-Plus), although balanced salt solution (BSS) may be closer to the optimal choice of BSS-Plus.
What is known about subject?
This is the only study that the authors know of comparing the irrigation in vivo effect of irrigating solutions and their effect on retinal electrical function with supporting histological evidence with parameters that closely replicate actual human surgery.
What are the findings?
All findings are new and novel in this study.
How might these results change the focus of research/clinical practice?
As cost containment of medical care continues, there will be further efforts to find less expensive and accessible replacements for solutions and drugs that we use during surgery. What this study shows is that some solutions (BSS) may be comparable with the ‘gold standard’ (BSS-Plus) that we now use, and some may not be (Lactated Ringers). This is very important in protecting the patient from uninformed cost-cutting, which may be driven purely by saving money at the expense of the patient’s care.
Introduction
Vitrectomy is the treatment of choice for posterior segment diseases that range from vitreous haemorrhage to malignant glaucoma. Machemer et al suggested using physiological saline for infusion in his original report.1 The metabolism of intraocular tissues like cornea, lens and retina depends on intraocular fluid composition, O2, pH, and osmolality. The best irrigating solution is important in achieving the best surgical outcome. The list of compounds in clinical or experimental settings started with normal saline. Solutions used include Lactated Ringers (LR), balanced salt solution (BSS) and balanced salt solution-plus (BSS-Plus). However, few in vivo studies compared the advantages/disadvantages of each of LR, BSS and BSS-Plus. Other solutions used in the past and experimentally investigated for use during vitreous surgery include Plasma-Lyte 1482, near physiological solution2 3 (see online supplemental tables), perfluorophenanthrene,4 perfluorotri-n-propylamine,5 polymethyl-3,3,3-trifluoropropylsiloxane-co-dimethylsiloxane,6 poly(2-hydroxyethyl acrylate),7 semifluorinated alkanes,8 silicone gel,9 methylated collagen,10 collagen/hyaluronic acid mixtures,11 hydroxypropylmethyl cellulose,12 crosslinked poly(vinyl) alcohol,13 polymethylacrylamidoglycolate methyl ester14 and crosslinked poly(1-vinyl-2-pyrrolidinone).15 However, in clinical practice, LR, BSS and BSS-Plus remain among the most commonly used solutions for vitrectomy. This study was a prospective, randomised, masked study. The aim of this study was to compare the effect of using three commonly used and commercially available types of irrigating solutions used during vitrectomy and their effect on postoperative electroretinogram and histology of operated animals compared with control eyes.
Animals and materials
Thirty-six New Zealand White male rabbits weighing 3–5 lb were included for the purpose of this study in all surgeries. Twelve rabbits were used for testing each of the three irrigating solutions, with a total of 36 eyes. Intraocular infusion solutions compared in this study were LR, BSS (Alcon Laboratories, Fort Worth, Texas) and BSS-Plus (Alcon Laboratories).
Anaesthesia
Ketamine (35 mg/kg) and xylazine (10 mg/kg) were used as intramuscular injection for induction of anaesthesia, and a second intramuscular dose of ketamine (l8 mg/kg) and xylazine (5 mg/kg) was given during surgery. Topical anaesthetic and pupil dilating eye-drops were instilled over the rabbit cornea and in the conjunctival sac before surgery.
Surgery
The eye was proptosed and passed through a slit cut in a piece of sterile glove to maintain the proptosed position. A two-port vitrectomy was performed by a single surgeon (HAD). The surgeon was blinded from the type of solution. Nasal and temporal sclerotomies, using a 19-g Micro Vitreo Retinal blade, 1.5 mm from the limbus at 10 and 2 o’clock positions were used. A 20-g vitrectomy cutter probe (Alcon Laboratories) was inserted into one sclerotomy wound and a 20-g infusion light pipe was inserted into the second sclerotomy. An axial vitrectomy with approximately 60% of the vitreous was removed, subjectively estimated. No lensectomy, posterior vitreous detachment or other surgical procedures were performed in any of the rabbits. No retinal detachments occurred. The irrigating solution was allowed to be infused for 5 min, and the eye was closed using sclerotomy plugs for 15 min periods. The fluids were kept at room temperature. This cycle of infusing the eye for 5 min and keeping the fluid for 15 min was repeated three times for a total operation time of 1 hour. A standardised bottle height that allowed for retinal and optic nerve perfusion was used during vitrectomy in all surgeries. In total, approximately 60 mL of infusion fluid at room temperature was passed through the eye during surgery. The sclerotomies were then closed with 7-0 vicryl sutures and the eyes were checked for normal intraocular pressure.
Electrophysiology
After the rabbits were anaesthetised, the pupils were dilated and topical anaesthetic was applied to the cornea. The animals were dark-adapted for at least 1 hour prior to recordings. The single bright flash electroretinography (ERG) was used. Many animals had preoperative ERGs, and the values of the preoperative ERGs were grouped so tightly that the 400 μV number was picked as the normal control reference value.
The ERG measurements were made at 2, 24 and 48 hours in all eyes. ERG measurements were also done at 6 and 72 hours postoperatively in some eyes. If the ERG had not returned to control values, additional ERGs were performed at 7 days and weekly thereafter. Dark-adapted ERGs were recorded by placing a cotton wick electrode on the cornea and a needle electrode on the skin above the eye. A ground electrode was attached to the ear. The electrodes were connected to a preamplifier with a half amplitude frequency set for a band pass of 0.1–2000 Hz. The output of the preamplifier was connected to an oscilloscope and to a computer for data storage. Stimuli were white light flashes of intensity setting of 16 for 10 min from a Grass instruments Model PS-22 photostimulator delivered at a rate of once per 3 min or longer in order to preserve the dark-adapted state between flashes. This stimulus is more than 5 log units above b-wave threshold; it was used to generate and record both a-wave and b-wave. ERGs were quantified by measuring the total ERG amplitude (a + b wave). The amplitude of the b-wave was measured from the peak of the a-wave to the peak of the b-wave. An ERG amplitude of 400 μV was considered a normal ERG as judged from preoperative normal control eye studies. None of the tested animals were diagnosed with surgical complications or an unusual postoperative course.
Histology
Biopsies were taken from the retina of 11 vitrectomised rabbit eyes 15 weeks postoperatively, and the retina was processed for H&E staining for histopathology.
Statistical analysis
Data were analysed using the Mann-Whitney U test.
Results
Electrophysiology
After analysing a number of ERGs (>10) from normal preoperative rabbit eyes, we observed tightly grouped values. We decided to establish a total amplitude (a-wave + b-wave) value of 400 μV as representing normal ERG amplitude. In subsequent experiments, we measured the time after surgery for the treated eyes to return to a normal (400 μV) level. Following vitrectomy and infusion with LR solution, all of these eyes had ERG values less than normal (around 36% of normal) at 2 and 24 hours (figure 1). After 48 hours and 72 hours, 1/12 (8.33%) and 3/12 (25%) of these eyes had normal ERGs, respectively. One week after surgery, 4/12 (33.3%) of these eyes had returned to normal levels. After 4 weeks, 6/12 (50%) of these eyes had normal ERGs and this number increased to 9/12 eyes (75%) at 10 weeks. In the remaining three eyes, no improvement in ERG amplitude was seen between 10 and 15 weeks, suggesting that these eyes were at their maximal improved level. In the BSS-treated and BSS-Plus-treated eyes, the ERGs recovered more rapidly after vitrectomy. At 2 hours, the amplitude of the recordings was reduced to approximately 35% of normal in all of these eyes (figure 1). A gradual increase in ERG amplitude was seen at 6, 24 and 48 hours postoperatively. At 24 hours, 4/12 (33.3%) of the BSS-irrigated and 6/12 (50%) of the BSS-Plus-irrigated eyes had normal ERGs. At 48 hours the number of rabbits with normal ERGs had increased to 8/12 (66.6%) in the BSS-irrigated group and 9/12 (75%) in the BSS-Plus-irrigated group. At 72 hours after vitrectomy, 12/12 (100%) BSS-Plus-infused eyes had ERGs with a total amplitude of 400 μV or greater, whereas 10/12 (83.3%) BSS-irrigated eyes demonstrated normal ERGs (figure 2). By 1 week, all (12/12) BSS eyes had also returned to normal. The statistical analysis of the effect of the three solutions on postoperative ERG in this report is based on total ERG (a+b wave) amplitude. Closer examination of the individual ERG recordings of the LR group revealed that the a-wave amplitude returned to a normal value in the majority of the eyes, even in the 25% of the LR-irrigated eyes where the total ERG amplitude had not returned to 80% of the normal value after 15weeks (figure 3). In conclusion, our results showed that differences between LR and BSS/BSS-Plus were statistically significant at 24, 48, 72 and 168 hours (p<0.05). No significant differences were found between BSS and BSS-Plus at any time point. However, looking at study rabbit eyes, the a-wave recordings showed that control a-waves had amplitudes around −180 μV previtrectomy. Twenty-four-hour postoperative recordings from each of the eyes had depressed a-wave values for all solutions used. Postoperative a-wave values for LR and BSS eyes were lower than for BSS-Plus eyes at 24 hours. These a-wave values increased over time back towards the control value of -180 μV in BSS-Plus and BSS eyes more rapidly than in the LR eyes.

Temporal changes in average ERG postvitrectomy as a percentage of Normal ERG relative to the intraocular infusion fluids. L-Ringers, Latacted Ringers solution; BSS, balanced salt solution; BSS-Plus, balanced salt solution-plus; ERG, electroretinography.
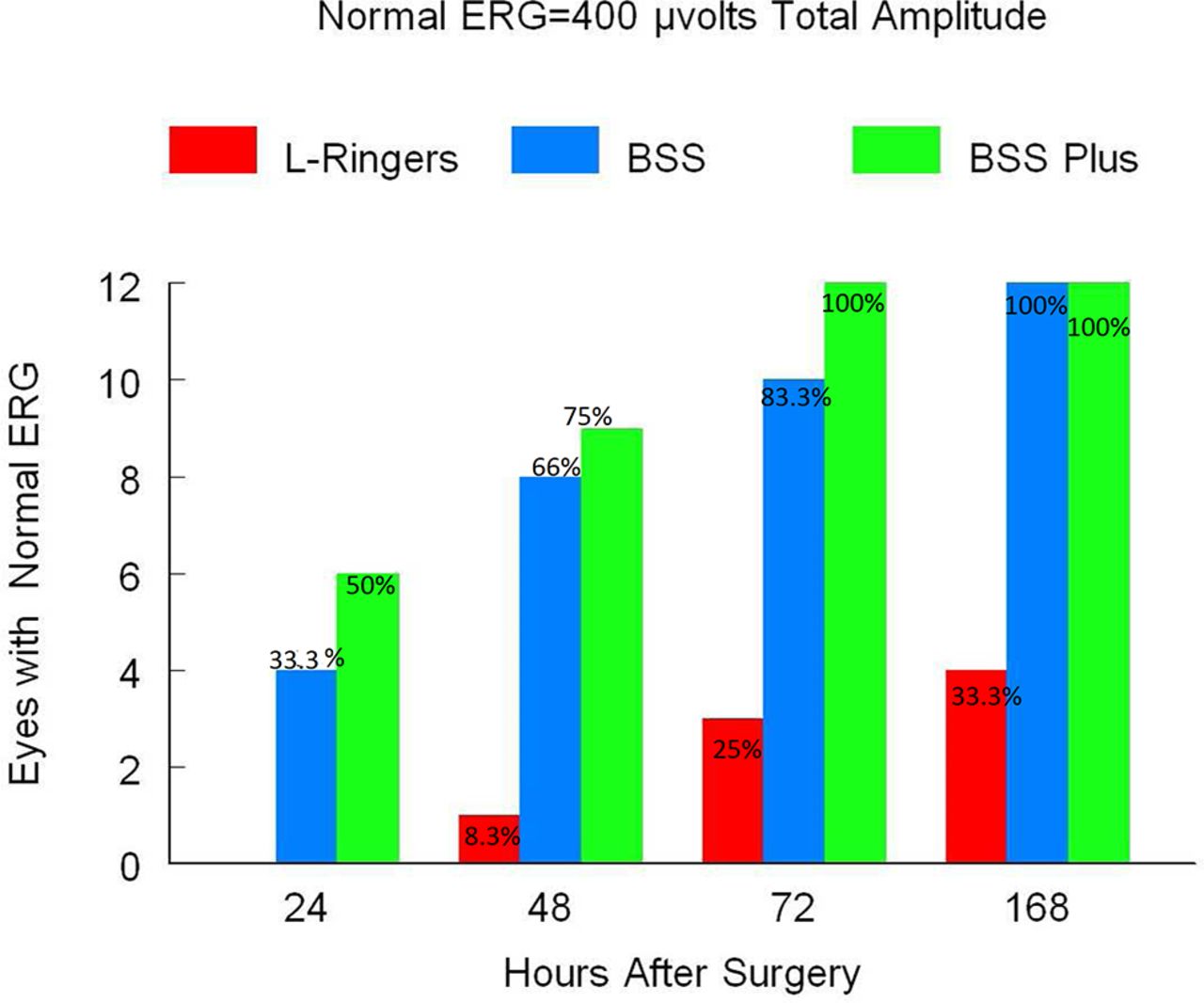
Comparing the number of rabbit eyes showing full recovery of ERG for each of LR, BSS and BSS-Plus in relation to time after surgery. L-Ringers, Latacted Ringers solution; BSS, balanced salt solution; BSS-Plus, balanced salt solution-plus; ERG, electroretinography.

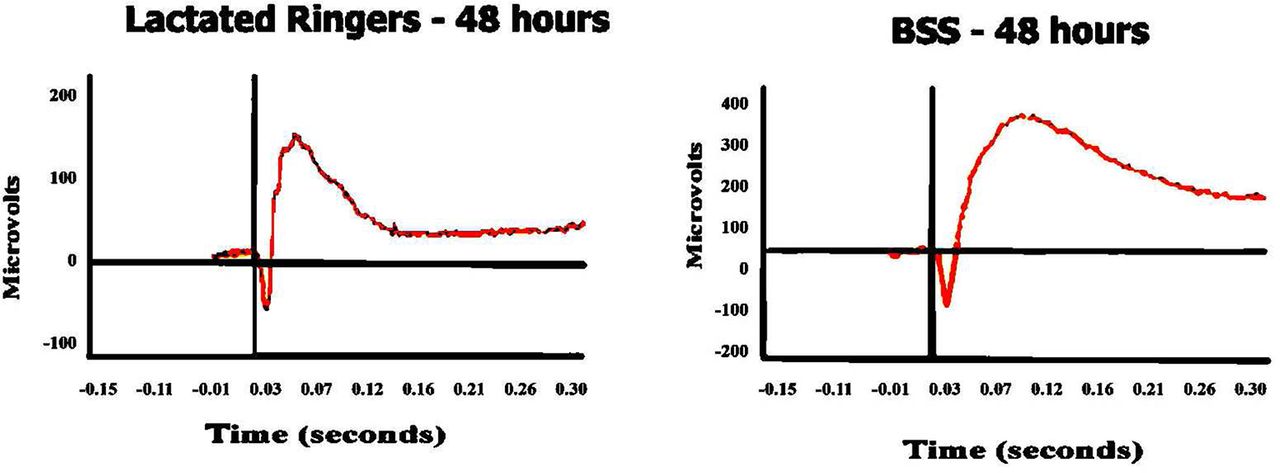
Sample ERG recordings. The left graph shows an LR-infused eye showing subnormal ERG (b-wave below 200 μV) after 48 hours. The right graph shows a normal amplitude ERG after 48 hours using BSS solution. BSS, balanced salt solution; ERG, electroretinography; LR, Lactated Ringers.
Histology results
The study included 11 rabbit eyes: 7 LR, 2 BSS and 2 BSS-Plus eyes. The retina biopsies were taken and fixed 15 weeks after surgery. In the LR eyes, 2 had normal retinas and 5 of 7 had histological changes in the inner and outer retina that included vacuolisation of either the inner or outer retina or both (figure 4) up to complete disruption. Each of the two retinas from BSS-irrigated and BSS-Plus-irrigated eyes demonstrated no gross histological abnormalities.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Photomicrograph of the retina of a vitrectomised rabbit eye. Lactated Ringers solution was used. There is vacuolisation within the inner and outer retina (arrows). ONL, outer nuclear layer specimens were stained with H&E.
Discussion
During a vitrectomy operation the extracellular milieu of the retina is changed due to perfusion of vitreous cavity and exposure of the inner retina to solutions that differ in varying degrees in ionic and metabolite composition compared with the physiological vitreous. Even the outer retina in many situations, as in cases of macular holes, rhegmatogenous retinal detachments, giant retinal tears and retinectomies are exposed to intraocular irrigation solutions. Retinal function and physiology are not expected to be altered significantly for a prolonged period after vitrectomy. A return to normal function is expected to occur quickly as vitreous is mainly water. Cells, proteins and solutes compose less than 1% of the vitreous. Many researchers have investigated how intraocular irrigation solutions may affect the retina. At the biochemical level, Winkler et al and Negi et al reported that bicarbonate is essential for normal retinal function. 2 ,16 Manzanas et al observed that intraocular concentrations of protein increased to nearly the same extent after vitrectomy in rabbits using BSS-Plus, saline and LR without a statistical difference between each solution.17 They also observed that lactic acid (assumed to be produced mainly by the retina) increased with saline and LR but not with BSS-Plus. Ascorbic acid was highest in the vitreous if vitrectomy was performed using saline as intraocular irrigating solution. Ascorbic acid levels were also high when using BSS-Plus rather than LR if measured during the early postoperative period. Manzanas et al suggested that BSS-Plus could be more harmful to the ciliary body at that time. They speculated that oxidised glutathione, present in BSS-Plus, contributed to oxidative damage, leading to higher synthesis of ascorbic acid by the eye in order to change the oxidised to the reduced form of glutathione. At the clinical level, Saornil and Pastor demonstrated that retinal oedema on early postoperative fluorescein angiography was increased when LR or normal saline was used more than when BSS-Plus was used for vitrectomy in rabbits. This oedema became more severe the longer the perfusion with the particular solution was maintained. However, they had a short follow-up and did not demonstrate how long this difference persisted.18 In our study, we investigated the effects of LR, BSS and BSS-Plus used as intraocular irrigating solutions on postoperative electrophysiology of the retina. Single bright flash (ERG) following at least 1 hour of dark adaptation was used to assess retinal function. We originally hypothesised that we would see a small difference among the three solutions, with BSS-Plus-irrigated eyes showing the fastest recovery. We were surprised at the length of time required for the LR-irrigated eyes to recover. It was even more concerning that some (25%) of the LR-infused eyes did not recover completely, even 15 weeks after surgery. Adding to the delayed recovery was the vacuolisation observed in these eyes on histological examination.
A significant decrease to 35% of a normal ERG (400 μV amplitudes) in a-wave and b-wave amplitudes was seen in all eyes when the ERG was recorded 2 hours after vitrectomy. This transient depression of ERG values noticed at 2 hours postoperatively with the three solutions can be multifactorial, with irrigating solutions, anaesthesia, or yet other factors that may not have been recorded and analysed in this report. Although there might be some differences in ERG response between rabbits and the eyes within the same rabbit, the sustained difference between test eyes and control value over our measurements minimised the significance of this phenomenon. In contrast, Moorhead et al reported that BSS-Plus-infused eyes demonstrated a smaller reduction in ERG amplitude than BSS-treated or normal saline-treated eyes. The magnitude of the decrease in ERG amplitude postoperatively was much larger in our study. This may be due to the increased time of vitrectomy (60 min vs 10 min). It may also be due to the larger surface area of retinacovered by only a thin cortical vitreous remnant which is exposed to infusion fluid current during the operation with our more complete vitrectomy technique, as compared to previous studies(single-port (Moorhead et al), vs. two-port vitrectomy in our study).
In this study, the serial postoperative ERG recordings showed gradual recovery. However, many of the ERG amplitudes returned to 90% of control values at 24–48 hours when using BSS and BSS-Plus. BSS-Plus showed an advantage over BSS at 48 and 72 hours, nonetheless not statistically significant. This is in agreement with the findings of Moorhead et al. By 72 hours, 83.3% of BSS and 100% BSS-Plus eyes had ERGs of normal amplitude. At 1 week, the ERGs of all eyes of these two groups showed normal values. In contrast, 1 of 12 of the LR-infused eyes had recovered to normal within the first 48 hours. Additionally, 75% of the LR eyes had recovered when measured 10 weeks after surgery. The remaining 25% of the LR-irrigated eyes had ERGs 20%–40% less than normal amplitudes even out to 15 weeks after vitrectomy. However, the authors could not explain why the SD in recovering LR eyes showed a tighter SD at 168 hours, similar to the level at 2 hours. It was expected that the data would be more disparate at 168 hours after surgery. Moorhead et al showed that postoperative ERG b-waves were better using BSS and BSS-Plus versus saline as intraocular irrigating solutions during vitrectomy in pigmented rabbits. BSS-Plus was best, however, not with statistically significant values. They reported that at 48 hours, normal saline-infused eyes had near complete recovery, with no statistical significance at 2 days postoperatively among the three solutions. This is in contrast to reports on biochemical effects, retinal oedema, and in vitro ERG depression associated with the use of normal saline in experiments previously performed: Negi et al; Manzanas et al; and, Saornil and Pastor.16–18 This is the first report, to our knowledge, on the in vivo effects of using LR as an intraocular irrigating solution. In this study LR was compared with the other most commonly used irrigating fluids in clinical practice (BSS and BSS-Plus). We also avoided any additional surgical procedures in contrast to cryopexy 2 weeks prior to vitrectomy reported by Moorhead et al. A prolonged vitrectomy time was applied (1 hour vs 10 min), closer to the actual vitrectomy surgery time. More vitreous (subjectively estimated 60% vs 30%) was removed, and two separate infusion and suction ports were used ensuring exposure of a wider area of retinal surface to the irrigating fluid solution. In Moorhead et al the investigators used a single infusion-suction-cutter probe with fewer animals.3 In our study, we also used 400 μV as an estimated normal ERG amplitude derived from preoperative eyes (recordings) as control. BSS-Plus contains bicarbonate, oxidised glutathione and glucose, and has a fixed pH of 7.4. These components were demonstrated to have a protective effect on corneal endothelium in previous studies (Benson et al and Waltman et al).19 20
However, attached retina is expected to be affected less by the type of intraocular irrigating fluid as diffusion through choroidal circulation remains a source of ions and metabolites. This is in contrast to corneal endothelium, whose supplies are restricted to the aqueous humour. We think that LR might have a permanent toxic effect on the retinal cells due to lower pH, higher lactic acid and lower osmolality. This might cause harmful retinal oedema, as previously reported by Manzanas et al, or some other type of damage to bipolar, Mueller or other inner retinal cells that contribute to the ERG b-wave.17 Our limited histological specimens corroborate our electrophysiological findings. This study is not free of some shortcomings: First, analysing b-wave and a-wave ratio and/or recording ERG using the International Society for Clinical Electrophysiology of Vision (ISCEV) standard would have been more informative, as we used total ERG amplitude for the analysis. It would have been better to include more serial histological examinations at different points of time. Further studies that include intraoperative ERG recordings and preoperative and postoperative retinal/choroidal optical coherence tomography recordings would also be more informative. In this report an axial vitrectomy was performed that removed around 60% of the vitreous, and there was a possibility that a peripheral layer of vitreous cortex was not removed in these rabbits, such that in this test environment any infusion fluid might only come into limited direct contact with the retina itself. In turn, the extent of the infusion fluid/retina interaction will be mediated by the residual cortical vitreous either through diffusion and/or hydration. To the best of our knowledge, the solution came into contact with the retina, although certainly not as much as if the posterior cortical vitreous were able to be removed. A much more direct contact between infusion fluid and retina in the human setting where the cortical vitreous has likely already been removed for the most part of any vitrectomy operation might lead to a more pronounced effect of the infusion solution.
In addition, studies comparing newer irrigating solutions are needed.
In conclusion, vitrectomy in a standardised experimental setting comparing three infusion solutions showed compromising effects on ERGs and retinal histology from LR solution infusion. The benefit of BSS-Plus solution over BSS solution infusion was less marked.
References
Footnotes
Contributors PF: gave the idea, shared in the primary planning/set-up and data analysis, supervised, read and helped in the corrections of the manuscript. GW: supervision, expenses, shared in manuscript revision and data retrieval. MH: shared in research plan and set-up, assisted in work, performed data acquisition, data statistical analysis and manuscript revision. HAD: performed surgeries, assisted in data acquisition, and wrote and submitted the manuscript. The previous persons are listed as authors of the manuscript.
Funding This research received no specific grant from any funding agency that involves any of the authors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.