Article Text

Abstract
Objective To study the effectiveness of amblyopia screening at ages 3–4.
Methods and Analysis From a population with no previous screening, a cohort of 2300 children with 3–4 years old attending school (91% of children this age attend school in Portugal), were submitted to a complete ophthalmological evaluation. Amblyopia was diagnosed, treated and followed. Amblyopia prevalence, treatment effectiveness, absolute risk reduction (ARR), number needed to screen (NNS) and relative risk reduction (RRR) were estimated.
Results Past/present history of amblyopia was higher than 3.1%–4.2%, depending on amblyopia definition normatives. Screening at age 3–4, had estimated ARR=2.09% (95% CI 1.50% to 2.68%) with a reduced risk of amblyopia in adulthood of 87% (RRR). NNS was 47.8 (95% CI 37.3 to 66.7). Treatment effectiveness of new diagnosis was 88% (83% if we include children already followed). 91% of new amblyopia diagnoses were refractive (of which 100% surpassed amblyopia Multi-Ethnic Pediatric Eye Disease Study criteria after treatment), while most strabismic amblyopias were already treated or undertreatment. Only 30% of children with refractive amblyopia risk factors that were not followed by an ophthalmologist, ended up having amblyopia at age 3–4. Eye patch was needed equally in new-diagnosis versus treated-earlier refractive amblyopia.
Conclusions Screening amblyopia in a whole-population setting at age 3–4 is highly effective. For each 48 children screened at age 3–4, one amblyopia is estimated to be prevented in the future (NNS). Screening earlier may lead to overdiagnosis and overtreatments: Treating all new diagnosis before age 3–4 would have a maximal difference in ARR of 0.3%, with the possible burden of as much as 70% children being unnecessary treated before age 3–4.
Involving primary care, with policies for timely referral of suspicious/high-risk preverbal children, plus whole screening at age 3–4 seems a rational/effective way of controlling amblyopia.
- public health
- vision
- epidemiology
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of the study
What is already known about this subject?
A screening should be thought as a programme that leads to the control of a disease and it may not be necessary if the disease is diagnosed and treated without it. Current evidence is insufficient to assess benefits versus harms of amblyopia screening in children younger versus older than 3 years old. As far as we could find in literature, there are no studies about the prevalence of amblyopia that could be diagnosed without a screening programme (ie, only with routine primary care) versus the prevalence of unsuspicious amblyopia by the age of 3–4 years. Number needed to screen (NNS), absolute risk reduction and relative risk reduction that are epidemiological measures used and published for many screening programmes worldwide, are still not reported regarding amblyopia screening.
What are the new findings?
We found that, screening amblyopia in a whole-population setting at age 3–4 is highly effective. For each 48 children screened at age 3–4, one amblyopia is estimated to be prevented in the future (NNS). Without a previous screening, if we look for the diagnosis only at age 3–4, treatment efficacy for new diagnosis was very high: 88% of the amblyopic children ended up with best visual acuity equal or higher than 0.7 in both eyes. Furthermore, we found that, screening earlier may lead to overdiagnosis and overtreatments: from 106 children with refractive amblyogenic risk factors that were not followed by an ophthalmologist, only 30% had amblyopia at age 3–4, raising the question if do we need to put all children under glasses, even though the majority will not develop amblyopia.
Significance of the study
How might these results change the focus of research or clinical practice?
We believe our study will be useful for policy and economic future planning, as well as future research planning, since it brought about the issue for the first time. Although we had some limitations to calculate the baseline risk (addressed in ‘assumptions/limitations’ sections) we believe we can still employ this valuable data used for many screening policies because, regarding amblyopia these objective measures were not described in literature yet. In the future, it would be better to have new studies using two samples to calculate the baseline risk, as in RCTs (randomized controlled trial).
Introduction
Amblyopia treatment has already been demonstrated as cost-effective.1 2 However, amblyopia screening strategies are still controversial.3 There are some contentious issues, such as screening and treatment efficacy in different age-screening models, which are crucial for planning policies.4 Absolute epidemiological measures are used to quantify the magnitude of effects of health interventions.5 The number needed to screen (NNS) is used to measure a screening programme effectiveness.6 Contrary to what the word might appear at first impression, NNS does not refer to the number of children that need to be screened to diagnose amblyopia. Rather, it is a dimension that incorporates treatment efficacy, since it is the reciprocal of the Absolute Risk Reduction (ARR). In amblyopia screening, NNS refers to the number of children that need to be screened to prevent one adult with amblyopia in the future, while relative risk reduction (RRR) is the percentage of baseline risk that is reduced by the screening. There are no reports about amblyopia NNS, ARR or RRR in literature, crucial for planning screening policies.
In this observational and prospective study, amblyopia was diagnosed, treated and followed. Epidemiological screening measures are estimated.
Patients/methods
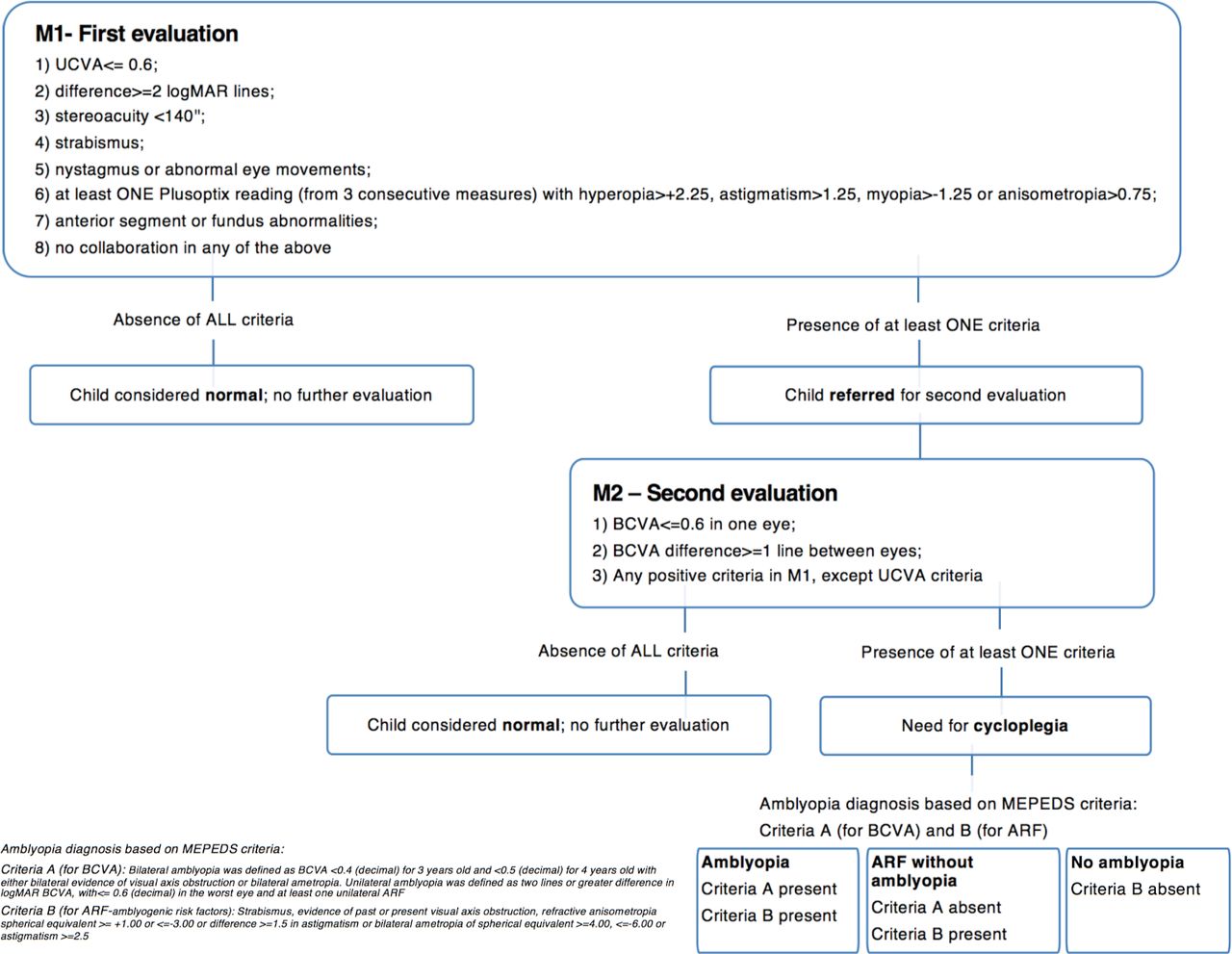
In a population of 3–4 years old with no previous amblyopia screening from the Northwest of Portugal, attending public and private schools (since in Portugal 91% of the children at age 4 attend school7, it covers almost all population), were brought to our Ophthalmology Department at Hospital de Braga, by our local government, for a complete eye examination. Participation rate was 96%. Methodology of each eye test performed was described earlier8 and are detailed in figure 1. We must emphasise that to avoid type II errors, judicious criteria were applied: children with any alteration in M1 were revaluated in M2 (figure 1); Plusoptix criteria to refer to M2 was based on NPV (negative predictive value) >98%9; This complete eye exam (M1/M2) left us, pragmatically, with no false negatives for amblyopia diagnosis.

Flowchart amblyopia diagnosis decision tree. Children were evaluated in M1 (moment one) accompanied by their school staff. Tests performed in M1 (evaluation without correction) included: uncorrected visual acuity (UCVA) with single-surrounding-tumbling-E; occular motility; cover-test; Plusoptix S04; Randot stereoacuity (circles); biomicroscopy; fundoscopy. If at least one criteria in M1 (see M1-box in flowchart) was present, they were called for further evaluation, M2 (moment two), this time in their parents’ presence. In M2, BCVA (Best Corrected Visual Acuity) was assessed and cycloplegia was performed when needed (see M2-box in flowchart). In the rare cases when children did not collaborate or their BCVA were not apparently congruent with their Amblyopia Risk Factors (ARFs), BCVA was re-assessed in another appointment, to ensure a correct amblyopia diagnosis. Note: ARF does not refer to Plusoptix screening criteria. ARFs were based on MEPEDS diagnostic criteria for amblyopia (detailed in fig 1) and refractive ARFs were considered positive only after cycloplegia. ARFs, Ambliogenic Risk Factor; MEPEDS (Multi-Ethnic Pediatric Eye Disease Study); UCVA, uncorrected Visual Acuity.
Children were divided in two groups (figure 2): (1) patients with amblyopia risk factors (ARFs) (subdivided in patients with and without amblyopia) and (2) patients with other abnormalities. Aetiologies were studied for each group.

Ophthalmologic findings in 3-4 years old children, in a previous unscreened population. Diagnosis of amblyopia and ARFs were confirmed by cycloplegia after a second evaluation. From 185 (8%) children with AFRs, amblyopia was found in 55 (29.7%), being the majority refractive and unilateral. See text for details. *ARF (amblyogenic risk factors) by MEPEDS: Strabismus, evidence of past or present visual axis obstruction, refractive anisometropia spherical equivalent >=+1.00 or <=-3.00 or difference >=1.5 in astigmatism or bilateral ametropia of spherical equivalent >=4.00, <=-6.00 or astigmatism >=2.5. **Amblyopia according to MEPEDS criteria: Bilateral amblyopia was defined as BCVA <0.4 (decimal) for 3 years old and <0.5 (decimal) for 4 years old with either bilateral evidence of visual axis obstruction or bilateral ametropia. Unilateral amblyopia was defined as two lines or greater difference in logMAR BCVA, with<=0.6 (decimal) in the worst eye and at least one unilateral ARF. ***Incomplete data or no collaboration. ****other problems-see text for details.
ARFs and amblyopia
Amblyopia and ARFs were defined by Multi-Ethnic Paediatric Eye Disease Study (MEPEDS) criteria (figure 2)10 and not by AAPOS criteria for amblyopia,11 because though similar to MEPEDS in BCVA, AAPOS ARFs criteria are not so clear (only ‘an amblyogenic factor needs to be present’11 prerequisite). Visual acuity (VA) is always reported in the decimal form.
Prospective study
Children with amblyopia were treated and followed. In the new-diagnostic cases, if, despite spectacles (mostly full correction), BCVA (best corrected visual acuity) stopped increasing, penalisation with eye-patch was added (penalisation hours was based on clinically accepted 2–4–6 hours/day, based on ATS-studies, and clinician could interchange regimens as needed). Amblyopia cases that were already under treatment, continued follow-up and treatment similarly. For all cases, BCVA was reassessed every 3 months until amblyopia resolved or BCVA stopped improving in three consecutive assessments. There were two main amblyopia outcomes for resolution: (1) normal BCVA achieved,8 when BCVA ≥0.7 in both eyes and difference between eyes <2 logMAR lines and (2) amblyopia surpassed, when MEPEDS BCVA criteria were surpassed.
Amblyopia screening effectiveness
Amblyopia treatment was considered effective when normal VA was achieved.
ARR represents the proportion of patients who, because of the screening programme, are spared the adverse outcome (amblyopia) in the future. It only refers to new diagnosis, since children already treated or under treatment are not influenced by the screening.
ARR=baseline risk* - final**
* baseline amblyopia prevalence, that is, without screening.
** final amblyopia prevalence, that is, after screening and treatment.
NNS refers to how many children need to be screened to prevent one amblyopic adult. Preventing one amblyopic adult means that a child was treated effectively and will not have amblyopia in the future.
NNS = 1/ARR
RRR refers to risk reduction in the context of baseline risk.
RRR=ARR/baseline risk.
Assumptions
To estimate NNS, since the sample that was given the intervention was the same sample used to estimate the control base event rate, the following assumptions had to be considered:
children reaching BCVA ≥0.7 in both eyes after treatment will remain without amblyopia in the future if they maintain follow-up.
Children with ARFs but without amblyopia will not develop amblyopia in the future, and if they do, it will be treatable, as long as they maintain follow-up.
Amblyopia not diagnosed at 3–4 years old will remain undiagnosed, untreated and unsolved.
Furthermore, we adjusted amblyopia BCVA criteria to our normative8 (percentile 1: BCVA≤0.4 at age 3 and BCVA≤0.5 at age 4), because leaving behind children with ‘normal’ BCVA by restrict MEPEDS criteria (BCVA <0.4 at age 3 and BCVA <0.5 at age 4), could bias the risk reduction in our cohort.
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
From 2300 children evaluated between May 2014 and December 2016: 1183 (51%)/1117 (49%) were boys vs girls; 1037 (45%)/1263 (55%) aged 3 vs 4. After re-evaluating children with criteria for M2 (n=528), ARF was confirmed to be present in 185 cases (figure 2); children with BCVA≥0.7 in both eyes, in the absence of ARFs were considered normal (n=1981); 120 children had other ophthalmological findings: biomicroscopy (n=37), funduscopy (n=15), ocular motility disturbances (n=68;10 with torticolis).
ARFs and amblyopia
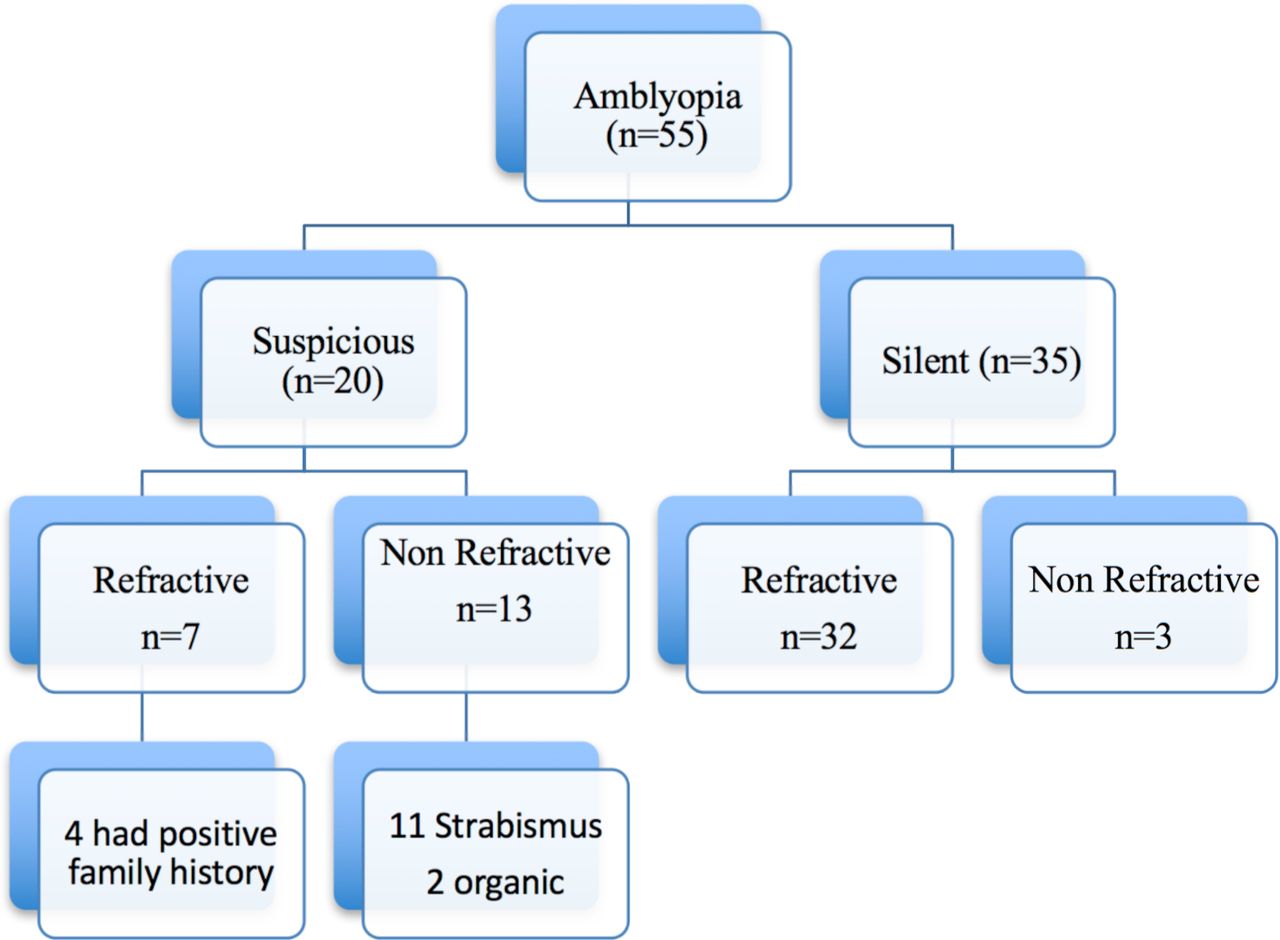
Amblyopia prevalence was 2.4% (n=55). In figure 2, amblyopia aetiologies are presented. In figure 3, we present which amblyopias were already under treatment and which were new diagnosis: from 36 children with a new diagnosis, 1 started manifest strabismus a few months prior and did not go for an appointment because was already enrolled in our programme (we considered that child as non-silent).
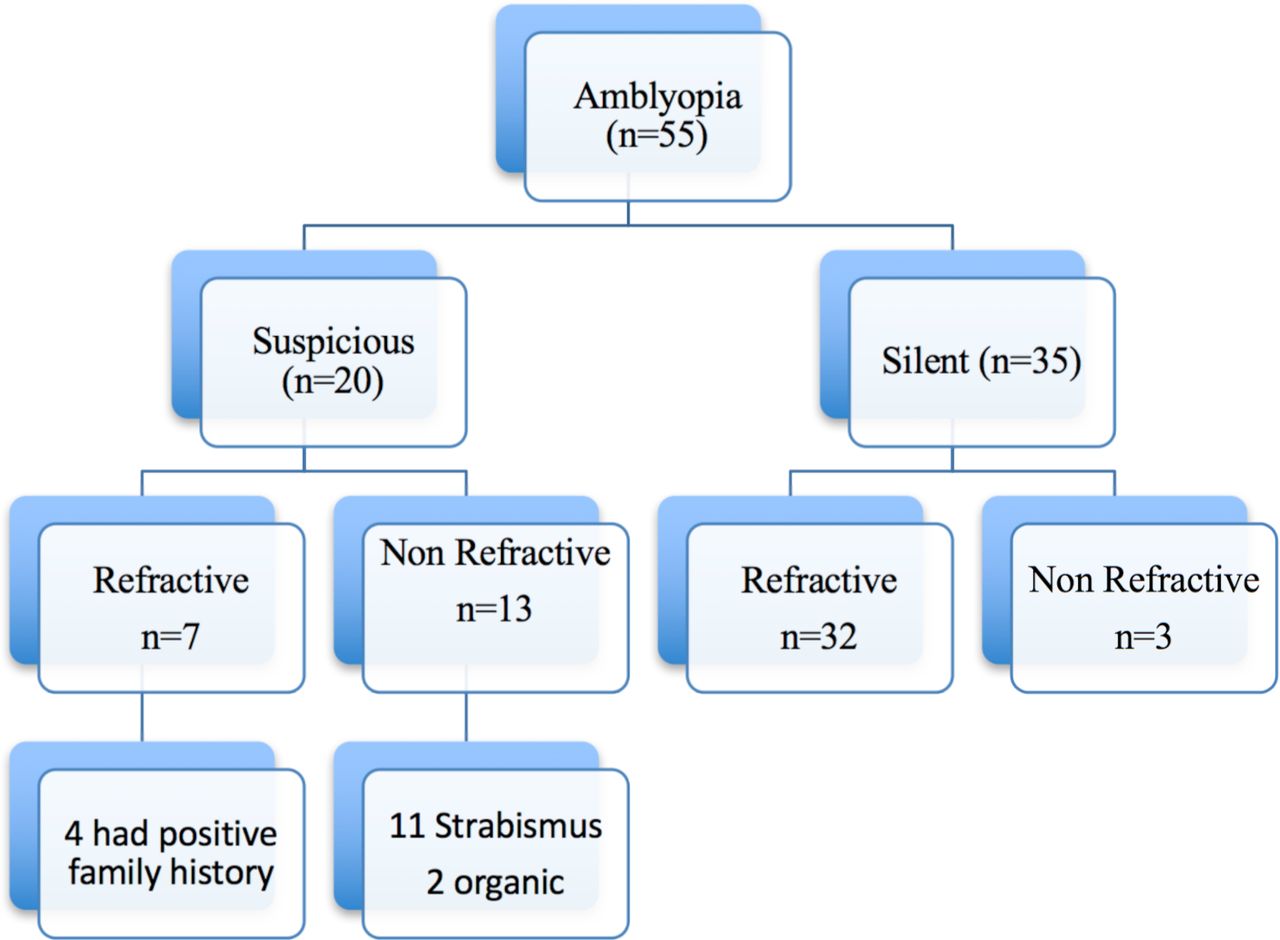
Ambyopias followed by ophthalmology (suspicious) vs. silent (unsuspicious, not followed by ophthalmology), in an unscreened population, at 3-4 years old: almost two thirds were silent amblyopias, 91% of which were refractive. Children with amblyopia already followed were mainly strabismic or with a positive family history for amblyopia, glasses or strabismus. See test for details.
Regarding previous history of amblyopia, we had 17 children with a presumed previous history: 9 had history of previous eye patch; 1 had bilateral IOL for ectopia lentis with prior known amblyopia; from 23 children with ARFs and a past/present history of glasses, 7 were presumed to have treated/prevented amblyopia (30% of the children with ARFs in this study turned out to have amblyopia). Past/present history of amblyopia was presumed to be higher than 3.1% (n=72).
Amblyopia treatment effectiveness
For amblyopia treatment effectiveness, we excluded eight children that were not followed by us. The mean follow-up of the 47 children (2.1%) enrolled with amblyopia was 14.27 months (SD=7.3): n=4 <6 months and n=21 >12 months follow-up. In table 1, we present treatment effectiveness of refractive versus non-refractive and new diagnosis versus previously diagnosed amblyopia.
Amblyopia treatment effectiveness
Eye patch was needed in 35.5% (11/31) of the children with newly diagnosed amblyopia and in 41.9% (18/43) of the children treated earlier. In refractive amblyopia, eye patch was equally needed (28.6%) in new diagnosis (8/28) and treated earlier (4/14).
Number needed to screen
After assumptions met (see methods), 79 children had amblyopia adjusting to our normative BCVA criteria, 54 were new diagnosis. ARR was 2.09% (95% CI 1.50% to 2.68%) and NNS was 47.8 (95% CI 37.3 to 66.7). ARR must be interpreted in the context of baseline risk, comparing with no screening (figure 4).12 Baseline risk was 2.39% (54/(2300-25-14)) and after screening it was reduced to 0.299% ((1-(54*0.875))/2261), with an RRR of 87.4%. Although we used our cohort BCVA normative criteria8 for estimating NNS, we also calculated the values using MEPEDS BCVA criteria to compare with future studies that might use that criteria: ARR=1.35% (95% CI 0.89% to 1.81%); NNS=74 (95% CI 55 to 112), for baseline risk=1.54%.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of event rate after screening (considering treatment efficacy of new diagnosis made at ages 3–4) versus base line event rate estimated based on the hypothesis of doing nothing, with the assumptions described in detail in text, we estimate an absolute risk reduction (ARR) and its reciprocal, that is, number needed to screen (NNS): for each 48 children screened at 3–4 years old, one amblyopia is prevented. Number needed to harm (NNH) was estimated comparing screening at preverbal ages (where abnormal BCVA cannot be assessed to confirm amblyopia diagnosis, assuming we would treat all ARFs by MEPEDS criteria) with screening at ages 3–4: For each 23 children screened in preverbal age, one is harmed. ARF, amblyopia risk factors; MEPEDS, Multi-Ethnic Pediatric Eye Disease Study. See text for further details.
Discussion
Risk reduction
When evaluating 2300 children at age 3–4, from a community based population, if we consider treatment effectiveness as reaching BCVA≥0.7 in both eyes, screening once at age 3–4 may reduce the risk of amblyopia in an adult by 87% (RRR), with ARR of 2.1%. For each 48 children screened, one adult with amblyopia is prevented in the future (NNS). Although with some limitations, it is the first report of these objective epidemiological measures regarding amblyopia screening. As recommended, ARR and NNS were calculated after excluding previously diagnosed/under treatment amblyopia,12 since the impact (the risk reduction) of a screening programme cannot include previously diagnosed children (it would give a higher, that is, better, but biased, ARR=3.0%).
In the present study, global amblyopia treatment effectiveness was 83%. In a cohort of 3216 children in Sweden followed from birth to age 10 years,13 amblyopia prevalence at age 4 was 2.9% and, at age 7, only 47% of those children achieved BCVA≥0.7 after screening and treatment.13 14 Those children were accessed at 1–3 days after birth for red reflex by a paediatrician, at 6–12 weeks and 6, 18 and 36 months for ocular media and alignment abnormalities by paediatrician or general practitioner and at age 4–5 VA (VA) was assessed by nurses. At that time, the author speculated14 whether evaluating VA at age 3 would change the scenario. As examinations done by our paediatricians/general practitioners since birth are similar to what was done in Sweden, and both studies have a high population participation rate, we think our better results could be attributed to one or all of the following: (1) diagnosing amblyopia at age 3–4 may lead to better treatment results, because of amblyopia earlier diagnosis; (2) VA assessment could have higher false negatives when done by non-eye professionals (in our cohort, 20% of all amblyopias had been considered normal by VA assessment by non-eye professionals prior to our evaluation); (3) the ‘post-PEDIG (Pediatric Eye Disease Investigator Group)-studies-era’ may permit amblyopia treatment with better compliance than 15 years ago; (4) in their study, not all children that achieved BCVA≥0.7 at age 4–5, maintained that VA at age 7–10. These questions should encourage future studies.
Moreover, our refractive amblyopia treatment effectiveness was 91%, and all children surpassed MEPEDS BCVA criteria, showing this amblyopia subtype has better treatment response. Furthermore, when looking at the children with non-refractive amblyopia, only four did not surpass amblyopia criteria, despite those four children were already under treatment before enrolment (two with strabismic amblyopia and two with organic amblyopia). For these reason, we speculate that screening earlier would not improve these values.
As a limitation to our assumptions calculating NNS: (1) we do not know if children with ARFs but without amblyopia, will develop amblyopia in the future, though we speculate that late-onset new-cases would be easier to treat; (2) some cases of amblyopia, not diagnosed at age 3–4, may still be diagnosed/treated/solved in the future (that may be our study main limitation) and (3) BCVA≥0.7 after treatment, may recur in longer follow-up, but we believe that, as these children should be kept under follow-up, if they recur, they will be treatable. NNS is time specific measure and our follow-up was only 14 months. Nevertheless, we believe it may not have relevant impact in NNS, since most new diagnosis, when screening at age 3–4, are refractive with low recurrence rates.
Prevalence of amblyopia and its risk factors
Amblyopia prevalence varies widely among different studies (0.6%–5.5%),11 because it depends on various factors.15 16 Besides population settings and the criteria applied, it also depends on the time of the diagnosis. In our cohort, amblyopia prevalence was 2.4%. We had 8% ARFs, what is lower than published for tertiary centres,9 as expected. However, if we adjust amblyopia prevalence to our BCVA normative previously published,8 amblyopia prevalence in 3–4 years old children was 3.4% (n=79), and at least 4.2% children had or have had amblyopia (n=96).
Refractive and strabismic amblyopia were not likely to be diagnosed the same way. Without a previous screening programme, 82% of refractive amblyopia were not followed at age 3–4 (and in all of those, parents said they did not intend to go to an ophthalmologist within the next year as they suspected nothing in their child), while most strabismic amblyopias were already under treatment. It seems that strabismic amblyopic children are sent to the ophthalmologist earlier, either because they develop signs perceived by paediatricians or primary care practitioners/parents, or because they belong to high-risk groups,11 with earlier referrals.
Regarding refractive versus strabismic amblyopia prevalence, we know from our hospital database that we have a ratio of 1.5:1.0,17 while in the present study, we have a ratio of 3.0:1.0 (ie, halved for strabismus). In a school basis population study in Portugal (children 6–11 years old), strabismus prevalence was 4%, also twice the 2.1% strabismus in the present study.18 We think these differences are due to two main causes: (1) from the 4% children that did not participate in our evaluation, many were already followed by an ophthalmologist, some with strabismus, according to their teachers and (2) Many strabismus are in syndromic and/or high-risk children who do not attempt school at age 3–4 and are already under ophthalmology and other hospital specialties follow-up; So, past or present history of amblyopia is possibly higher than 4.2% described above, showing the magnitude of amblyopia and the need to address it as a public health problem.
Although 0.7% children, without amblyopia, needed a second evaluation because of fundus findings, all revealed to be minor findings, for which we speculate that fundus screening at age 3–4 years, in a whole-screening population basis, may not be necessary.
Harms
If screening was before age 3, when collaboration in VA to confirm diagnosis is difficult, and while there is no technology that helps us to accurately diagnose amblyopia in pre-verbal children, assuming we would treat all ARF, number needed to harm (figure 4) would be 23 for an attributable risk of 4.4% based on children we would need to overtreat (children with ARFs that at age 3–4 had no amblyopia and were not followed by ophthalmology yet). That means that for each 23 children screened before 3–4, one child would be unnecessarily treated. Whether that children will or not develop amblyopia in the future, is a pertinent question for future studies.
Harms of screening come from three different aspects of a screening programme: overdiagnosis, incidentalomas and false positives. Amblyopia screening before age 3 leads to an increase of all these three aspects. ‘Get tested, diagnose disease early, and be treated while the problem is ‘small’ before it becomes ‘big’.19 In short, harms are the result of both looking harder (more screening leads to more ‘diagnosis’) and lower thresholds for a positive diagnosis (technology and medical advances).19 Amblyopia overdiagnosis means a child is diagnosed with amblyopia, treated as amblyopic, but that disease, if left untreated, would never had any impact in that person’s life. It means children wearing glasses, eye patches or eye drops they may not need. Those over treatments may (or not) have impact in children’s health, either social interaction, psychological harms or even emmetropisation.20–28 All these aspects should be studied carefully in the future.29 30 Screening only after 3 years old, means we can confirm presence of amblyopia in children having both ARF and abnormal BCVA. ARF is not always equal to amblyopia, either in refractive or strabismus, even if assessed indirectly through preference looking in the later.31
The major randomised trial32 favouring universal earlier screening should be interpreted with caution. They compared amblyopia prevalence at age 7.5 in two groups: children submitted to an intense vision screening at 8/12/18/25/31/37 months (n=1088) vs a one-time-screen at 37 months (n=826). Although they found no difference in amblyopia prevalence for unilateral amblyopia (which is by far the most prevalent type), they favoured the intense earlier screening based on the differences found in prevalence of VA≤0.4 in the worst eye (0.63% vs 1.81%, p=0.02). However, for their sample (n=1914), the χ2=5.6, with one degree of freedom reported, we calculated an r-based effect size: r2=0.0029. That means that only 0.29% of their statistically significant results are explained by the different kind of screenings. We did the same regarding unilateral amblyopia (although they reported non-significance with p=0.06) and we obtained an effect size of 0.0018. Since small little differences can be found as statistically significant when we increase sample sizes, p values must always be interpreted with care, and effect size is mandatory to establish clinical significance. Furthermore, if a child at age 7.5 has the worst seeing eye<=0.4, it implies having unilateral amblyopia in most cases. These results, in our perspective, show no clinical significance.
Hypothetically theorising that treating all our new diagnosis before age 3–4 would lead to all those children with BCVA>=0.7 (what might be an excessive speculation), screening before age 3–4 would have a maximal difference in ARR of 0.3%, with the possible burden of as much as 70% children wearing unnecessary glasses before age 3–4.
Finally, although not being a screening programme, but rather a complete eye examination, the present study gives valuable information for future screening programmes and policies. If a high-sensitivity screening method is provided (which should be looked at in future studies to avoid this complete examination), screening at ages 3–4 is highly effective. Using lower sensitivity screenings may not lead to the same outcomes.
In conclusion, diagnosing and treating amblyopia at ages 3–4 (in a whole-population setting, without a previous screening programme) is highly effective. This study reinforces the current evidence that amblyopia screening in a whole-population setting before age 3 may not be necessary. Basic ophthalmological evaluations by primary care (red reflex since birth, plus cover test and corneal reflexes), as well as recognising high-risk children need to continue and be encouraged since they result in earlier high-risk children referrals
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
Written informed consent approved by Human Research Ethics Committee of Hospital de Braga adhered to the tenets of the Declaration of Helsinki and was obtained from parents/guardians before first evaluation (M1).
Acknowledgments
We thank Dr Fernando Vaz, Head of Ophthalmology Department of Hospital de Braga, and Dr Ricardo Rio, Mayor of Braga Municipality, for their support in the implementation of this project in Hospital de Braga that gave all 3–4 years old children the opportunity for an eye examination, with social equity—without the need of parents to miss work to accompany their children. To the other Mayors of the five municipalities that joined the project afterwards.
References
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors SG conceptualised and designed the study, designed the data collection instruments, acquisition of data, carried out analyses and interpretation of data, drafted the initial manuscript, and reviewed and revised the manuscript. AS, CF, RDL and PB collected data and revised the manuscript critically for important intellectual content. PSC and EDS conceptualised the study, carried out interpretation of data and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.