Article Text

Abstract
Objective To present an established practice protocol for safe and effective hospital-setting ophthalmic practice during the coronavirus disease 2019 (COVID-19) pandemic.
Methods and Analysis Literature was reviewed to identify articles relevant to COVID-19 pandemic and ophthalmology. The following keywords were used: COVID-19, SARS-CoV-2 and telemedicine, combined with eye, ophthalmology, conjunctivitis and tears. Data were extracted from the identified manuscripts and discussed among subspecialists to obtain consensus evidence-based practice.
Results A protocol for ophthalmic practice in the era of COVID-19 pandemic was established. The protocol covered patient screening, clinic flow, required personal protective equipment and modifications of ophthalmic equipment for improved safety.
Conclusion Important literature emerged with respect to the practice of ophthalmology in the era of COVID-19. An evidence-based ophthalmic practice protocol was established and should be modified in the future to accommodate new insights on the COVID-19 pandemic.
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Coronavirus disease 2019 (COVID-19) is an ongoing pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
The virus spreads mainly during close contact and by small droplets produced when an infected patient coughs, sneezes or talks.
Ocular surfaces may be a potential mode for transmission, and ophthalmologists are highly prone to getting infected.
Several infection control measures have been universally recommended.
What are the new findings?
Our aim is to discuss the consequences of the COVID-19 pandemic on ophthalmology practice in the setting of a referral hospital.
The diagnosis of COVID-19 in one of the ophthalmologists in our department prompted epidemiological investigations and tightening of the protocols based on relevant literature and guidelines.
How might these results change the focus of research or clinical practice?
This experience may help other colleagues to overcome the current ordeal with minimal unfavourable consequences.
Introduction
The WHO has declared coronavirus disease 2019 (COVID-19) as a public health emergency of international concern.1 It was concluded that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes COVID-19, spreads primarily through droplets of saliva or discharge from the nose when an infected person talks, coughs or sneezes. It is transmitted from person to person who are in close contact (within about 1.8 meters). Furthermore, it is possible that the virus transmits by touching a surface or an object that has virus-containing respiratory droplets, and then touching the eyes, mouth or nose.2 3 This mode of transmission may be important as coronavirus has been isolated from surfaces several days from dissemination.4
As the percentage of SARS-CoV-2-positive cases increases, affected patients might frequently present to eye clinics or emergency departments.5 When patients come to an ophthalmologist office for ocular examination, these patients have direct contact with examination equipment. A recent report by Lu and colleagues3 suggested that ocular surfaces may be a potential mode of SARS-CoV-2 transmission and that ophthalmologists are highly prone to getting infected. Lai et al 6 reported infection control measures which were based on a three-level hierarchy of control measures: the use of personal protective equipment (PPE), environmental control and administrative control. In addition, pandemics may potentially accelerate moves towards telemedicine, by which patients are treated by doctors and nurses remotely.7 8
Our aim is to discuss the consequences of the COVID-19 pandemic on ophthalmology practice in the setting of a referral hospital. The diagnosis of COVID-19 in one of the ophthalmologists in our department prompted epidemiological investigations and tightening of the protocols based on relevant literature and guidelines. A practice protocol was established including infection control measures and several significant modifications of daily work to minimise infection of both the eye care providers and the patients.
Methods of literature search
Literature search was conducted in PubMed and Google Scholar databases. Several search terms were used, including coronavirus, SARS-CoV-2, COVID-19, ophthalmology, ophthalmologist, tears, conjunctivitis, telemedicine in ophthalmology and their combinations. Only abstracts in English were reviewed, and the full publication of manuscripts that were judged to be relevant was retrieved. When relevant, publications cited in articles selected by the search were also retrieved. No restrictions were applied with regard to date of publication.
Recommendations of the American Academy of Ophthalmology (AAO), WHO, the Centers for Disease Control and Prevention (CDC), the American Society of Retina Specialists, the Israel Ministry of Health, and the Israeli Ophthalmological Society (IOS), for safe practice during the COVID-19 pandemic, were also reviewed.
Patient and public involvement
Patients were not involved in this research.
General considerations
Several infection control measures were universally recommended, and few manuscripts have detailed experience gained during the ongoing coronavirus epidemic and previous epidemic outbreaks.6 9 10 Infection measures were subdivided into three categories: the use of PPE, environmental control and administrative control. In addition, the use of telemedicine was encouraged to provide care for non-urgent cases.11 12
Personal protective equipment
The AAO5 and IOS13 have published a report advising ophthalmologists to wear masks and eye protection when caring for patients potentially infected with COVID-19. Anecdotal reports suggested that when no eye protection was worn, COVID-19 could be transmitted by aerosol contact with conjunctiva.3 5 14 In addition, patients should be requested to refrain from speaking as much as possible during the slit lamp examination. Furthermore, ophthalmology practices in Hong Kong10 recommended use of PPE for all cases regardless of SARS status, as well as hand hygiene measures and use of gloves, N95 masks, goggles and gowns.
Environmental control
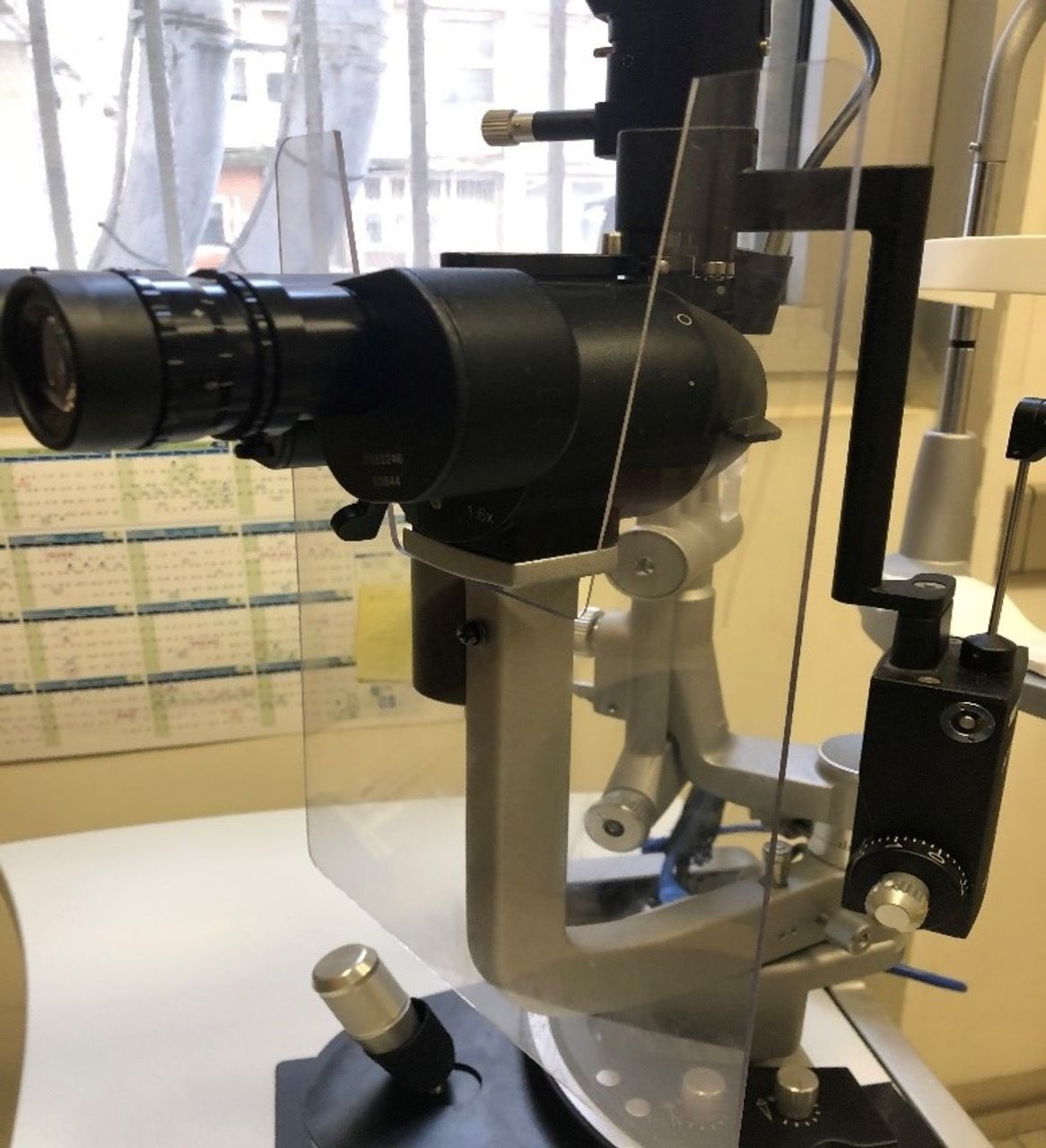
Installing large protective plastic shields on slit lamps to minimise the risk of droplet contamination between the patient and the ophthalmologist was widely performed. The IOS and AAO5 also recommended such installation (figure 1). Disinfection of instruments including slit lamps, controls, accompanying breath shields and tonometer tip, keyboards, desks, door handles and chairs after examination of each patient must be performed. Other shared equipment such as the B-scan probe and contact lenses for photocoagulation needs strict sterilisation protocols as well.5 6 The CDC15 recommended the use of disinfectants specific to COVID-19, including diluted household bleach (five tablespoons of bleach per gallon of water) and alcohol solutions with at least 70% alcohol. Lai et al 6 reported the importance of air ventilation in waiting areas and suggested opening the fresh air dampers of the air handling equipment to achieve higher rate of fresh air with improved air dilution.
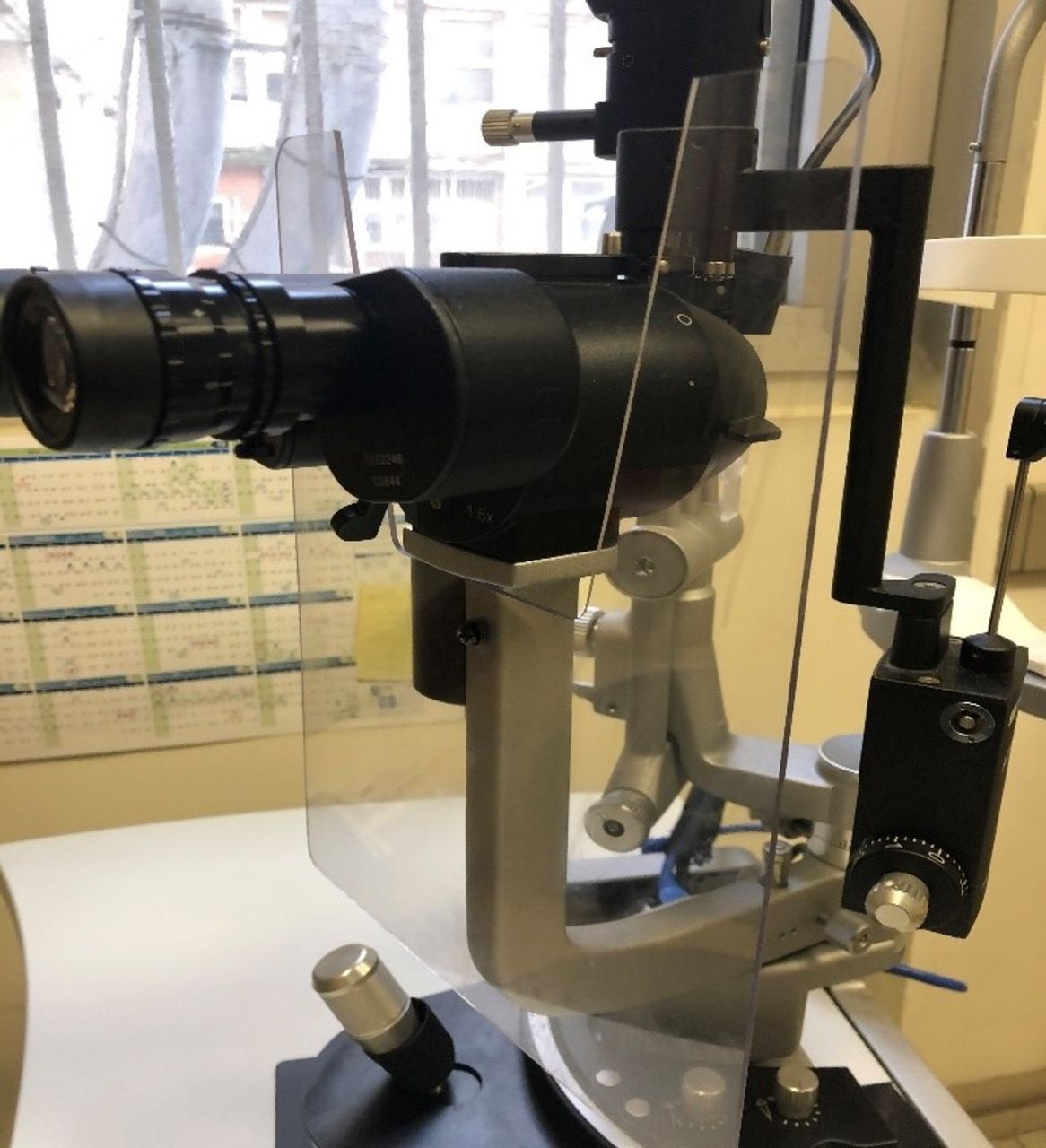
Enhanced plastic breath shield.
Administrative control
Basic survey to identify patients with possible exposure to SARS-CoV-2 or the development of COVID-19 should be performed. This should include questions about symptoms (fever, dry cough, sore throat, headache, loss of taste/smell) and proximity to a validated or suspected COVID-19 case as well as travel to an endemic region.5 13 16 For patients who meet these criteria, immediate notification should be sent to both the infection control personnel at the healthcare facility and the local or state health department for further investigation of COVID-19. The patient must then be referred for appropriate care. Preferably, such screening should be performed by calling the patient in advance, as well as at the front desk once the patient arrives at the clinic.
Balancing between the need to provide care and save sight and the risk of contracting COVID-19 should be considered with respect to each patient. Generally, elective visits and surgeries should be postponed. Medical care should be provided only to urgent cases. A triage procedure should be performed to identify patients who should be urgently or emergently seen by the ophthalmologist versus those who may benefit from telemedicine or internet-based visit and those who may be safely rescheduled.
The WHO17 launched a case classification scheme which triaged patients into healthy, suspect, probable and confirmed COVID-19 categories. The Israel Ministry of Health, IOS and Seah et al 9 13 16 reported that in an ophthalmic emergency, all categories except healthy individuals with an eye condition should be seen in an isolation ward depending on the relevant guidelines and protocols. In addition, efforts should be invested to prevent crowding of waiting areas. For that purpose, social distancing was implemented in waiting areas by blocking alternating seats (figure 2).

Waiting area.
Telemedicine
Telemedicine is defined as the use of information technologies to support healthcare between participants who are separated from each other.12 It represents a combination of expertise and technology that delivers medical services and information over distance.11 The use of telemedicine in ophthalmology was first described in 1999 by HK Li,11 where he touched briefly on the ways in which this new tool might profoundly alter the professional landscape and the practical aspects of setting up ophthalmic telemedicine centres.
A concern has been previously expressed that telemedicine could be disorienting for patients, who might find themselves ‘objectified’.18 However, many patients seem open to electronic encounters. The younger generation, accustomed to teleconferencing and smartphone photo or video interactions, is likely to be comfortable with such interactions.19 Fortunately, the current work environment is highly advanced in technology, with video-equipped computers, high-resolution cell phone cameras and fast broadband internet service all in place.
Disasters typically lead to a surge in demand for medical care that overwhelms local capabilities. Telehealth can help manage the surge in visits that result from injuries, exacerbations of chronic conditions and closure of outpatient offices.20
Structured reorganisation during the COVID-19 pandemic
Based on the recommendations of the WHO, CDC, AAO, Israel Ministry of Health and IOS and relevant manuscripts,5 13 16 21–24 several specific measures have been undertaken while keeping PPE and environmental and administrative controls in our priorities.
Triage for patients and encouraging the use of telemedicine
Individuals with non-urgent ophthalmic problems who were suspected, probable or confirmed COVID-19 cases were referred for medical treatment. If the visit was urgent, they were evaluated in a designated isolated clinic at the emergency department.
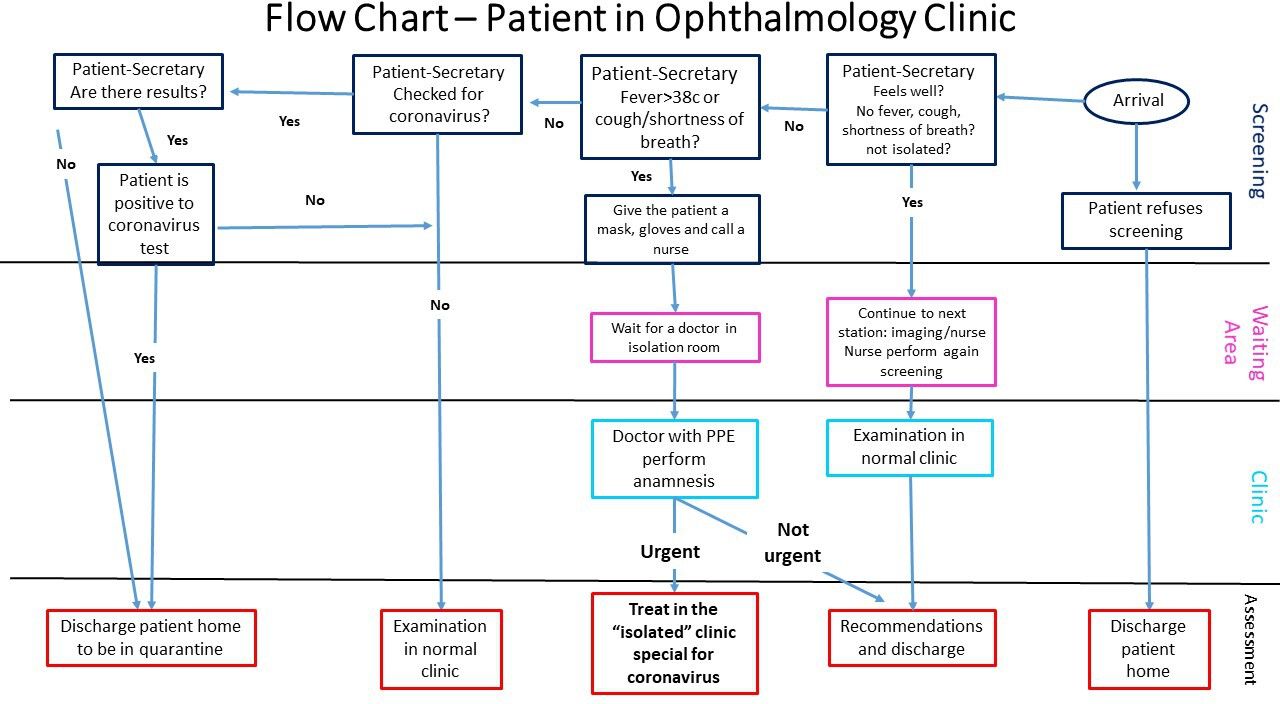
Regarding presumed unaffected individuals who were authorised to come to clinics, flow charts were developed that refer moderate-risk to high-risk patients to nurse triage, who asks each patient regarding their risk for COVID-19 through a questionnaire (figure 3).
{kind=link}
{kind=link}
{kind=link}
Flow chart of patients in ophthalmology clinics. PPE, personal protective equipment.
Video examination visits and remote telephone-based interviews were set for non-urgent patient visits to try to reduce direct patient–physician encounter.
Dividing workers into teams and departmental meetings
Doctors and nurses were divided into small fixed teams that worked separately and in different shifts as much as possible.25 Each such team included at least one attending physician. Consultations with other physicians were performed via phone. Alternatively, if examination is required, the consulting ophthalmologist entered the room only after the previous examiner has left the room. This measure was undertaken to prevent cases of infected coronavirus staff member exposing other colleagues to coronavirus and the need, as a result, for isolating large numbers of staff members.26 27
Academic and administrative meetings and lectures were conducted by online applications. Face-to-face meetings or lectures were cancelled.
Separated imaging areas
Imaging service provided scans for urgent patients using modified shortened imaging protocols in order to provide rapid and minimal contact with patients.28–30 Imaging devices were placed in different rooms. If possible, an optical coherence tomography (OCT) device was allocated to the designated isolated examination room for imaging a patient suspected of COVID-19.31
Surgery service and hospitalisations in ophthalmology ward
Elective surgeries were cancelled. Only urgent cases were approved, while keeping infection measures protocol.
Hospitalisations were authorised for coronavirus-free cases that needed urgent hospitalisation and treatment. Suspected or probable cases were evaluated for COVID-19, and if positive they were admitted to a designated department, along with confirmed cases.
Check-up coronavirus tests for staff members
Staff members suspected of developing COVID-19 based on contacts with presumed or confirmed patients or if they have developed symptoms suggestive of COVID-19 were immediately quarantined and tested to rule out SARS-CoV-2 infection. Two separate negative PCR tests within 48 hours were performed prior to returning to the clinic. Quarantine for 14 days from last contact was imposed in cases of contact with a confirmed case.
Specific measures for subspecialties
Paediatric ophthalmology service
Paediatric ophthalmology services were shifted towards telemedicine when possible. Telemedicine is widely used in paediatric ophthalmology for general screening for amblyopia, refraction and motility disorders,32–34 as well as for retinopathy of prematurity (ROP) screening.35 36 Several components of the paediatric ophthalmological examination can be performed at home by guardians: visual acuity for near and distance can be measured using web-based applications. Using a printed chart and measuring the symbol size may control for hardware and software variations. This information is sufficient for treatment decisions for older children who are being treated for amblyopia. Parents can be instructed to perform basic eye movement examination and send a simple video, or use dedicated computer or phone applications, assisting with poststrabismus surgery examinations and other ocular movement disorders. Unfortunately, examination of the anterior and posterior segments of the eye requires either a professional or an expensive imaging instrument. The use of web-based refraction systems on paediatric patients is unreliable at this point due to calibration and validation issues. The presence of a good red reflex with good visual acuity and alignment may suffice to screen most healthy children until full examination is possible.
Most patients who had follow-up appointments for refractive errors, strabismus or amblyopia were advised over the phone and their clinic visits were postponed. Appointments are considered urgent when vision is at risk, mostly due to amblyopia in a young child. All patients under 8 years old who have cataract, premature babies for ROP screening, patients with active uveitis and glaucoma, as well as recent postoperation cases were seen in the clinic.37
Surgeries under general anaesthesia pose additional risk for the staff, as endotracheal intubation generates aerosol.38 All non-urgent interventions, such as strabismus surgery, were postponed. Urgent cataract surgeries in younger children, retinal procedures and trauma-related surgeries were performed if the anaesthesia-related facilities could maintain this service.
Neuro-ophthalmology service
The neuro-ophthalmology service adopted a protocol mandating that all consultations begin with a remote telephone-based interview. The utility of telemedicine has been established in neuro-ophthalmology for many years.39 Neuro-ophthalmology is particularly amenable to telemedicine because a detailed history can often lead to a diagnosis. For example, a recent study demonstrated that an experienced neuro-ophthalmologist could correctly diagnose 88% of new cases based on the history alone.40
Beyond the patient’s history, many aspects of the physical examination can be performed through simple photographs and video that patients can obtain using their smartphones. Anisocoria can be assessed by asking the patient to photograph their eyes in dim and bright light. Videos can allow assessment of strabismus and nystagmus.
In some cases, the above assessment will clearly indicate that the immediate course of action should be referral to the nearest emergency department.41 Sometimes, it will be apparent that the clinical circumstances are not urgent, allowing for the neuro-ophthalmology examination to be deferred. In some circumstances, it may become apparent that the indication for a neuro-ophthalmology assessment was not even justified (eg, monocular diplopia).
When the steps described above leave clinical ambiguity, a direct patient–physician encounter may still not be immediately necessary. Specialised tests can be performed, which the neuro-ophthalmologist can assess remotely. These include automated visual fields, OCT and neuroimaging. Digital fundus photography has allowed for neuro-ophthalmologists to telemedically diagnose both optic disc oedema42 and optic atrophy.43 OCT is becoming an increasingly accessible imaging alternative for the optic disc and has even been shown to be more sensitive than direct ophthalmoscopy in the diagnosis of optic disc abnormalities.44
Retina service
The retina clinic has a large component of patients who are elderly and with comorbid diseases. New measures were adopted in treating retina patients to reduce their exposure to each other and to the medical team as much as possible.
Patients with urgent sight-threatening conditions (eg, retinal tears, retinal detachments, trauma and so on) should be examined and treated through the emergency room. Appointments for all non-urgent patients were cancelled (eg, patients with epiretinal membranes, more than 6 months of follow-up since vitreoretina surgery and all patients with retinal dystrophy).45
Anti-vascular endothelial growth factor (VEGF) therapy is provided under a modified regimen.25 45 46 Each day different teams of injecting retina specialists, nurses and residents are present at the clinics, with a minimum number of staff possible; teams scheduled on different days should not meet each other.25 Patients treated with anti-VEGF may be triaged to identify those where treatment can be delayed.
Patients under monthly intravitreal injections continued to receive the injections as planned in their last visit to the clinic. Visual acuity assessment and clinical examination may be postponed, and treatment decision may be based on OCT findings. OCT images may be reviewed by a retina specialist at home with a remote connection,47 who decides on the interval of injections for each patient following a treat and extend protocol.
Telemedicine has been suggested as the innovative solution to provide care for patients with diabetic retinopathy (DR), as it allows evaluation of DR in the primary care setting using digital fundus images, which are evaluated remotely by trained graders. Ocular telehealth programmes for DR can effectively diagnose sight-threatening DR in the primary care setting and recommend appropriate care interventions.48 49 The use of telemedicine has been described also for evaluation of other retinal abnormalities such as acute floaters and age-related maculopathy.50 Yet improved home-based retina imaging is a major limiting factor in increasing the reliability of home-based monitoring.
Cornea service
COVID-19 may cause external surface disease. Conjunctival congestion was documented in 9 out of 1099 (0.8%) patients with laboratory-confirmed COVID-19 from 552 hospitals in mainland China.17 A small study on 30 patients with confirmed COVID-19 aimed to elucidate the presence of SARS-CoV-2 in tears and conjunctival secretions of infected patients by collecting the samples twice at intervals of 2–3 days. Only one patient who had conjunctivitis was found to harbour viral RNA in the tear fluid and conjunctival secretions twice. The conjunctivitis was characterised by conjunctival congestion and watery discharge. The patient had no severe fever or respiratory symptoms when the specimens were collected, and the disease was in its early stages. No viral RNA was detected in the tear fluid and conjunctival secretions of the other patients without conjunctivitis.16
Although somehow limited without the help of a slit lamp or an attachable optical aid, patients scheduled to the cornea clinic were offered to undergo telemedicine consultation using their smartphone camera. The doctor reviews the photo and asks the patient about symptoms such as change in vision, photophobia, pain, redness, secretions, the number of artificial tears needed or any unusual relevant symptoms.47 51
Examples of urgent cases that need to be examined in the clinic include active keratitis of any sort, corneal ulcers, corneal perforation or melt, corneal graft rejection, and foreign bodies that necessitate removal. In any of these cases, patients were instructed to visit the clinic with maximal personal safety measures, alone if possible, and with at least half an hour gap between patient visits.52
Non-urgent cases such as keratoconus follow-up after ultraviolet corneal cross-linking or stable keratoconus, postkeratoplasty patients especially 3 or more months after the surgery, dry eye, and resolved keratitis are instructed to adhere to the standard treatment protocols considering their last clinic visit via a telemedicine visit.
All elective surgeries were postponed until further notice. Even keratoplasties were considered elective surgeries and were not performed routinely, but our cornea harvesting team was instructed to keep two viable corneal grafts in cold storage (5°C) for any case of emergency keratoplasty, for example ‘therapeutic penetrating keratoplasty’ in a case of severe keratitis leading to corneal melt and perforation.53 The donors were also tested for COVID-19 during the organ harvesting process, although ocular transmission is in doubt.54 55
Uveitis service
Patients were contacted via phone and instructed to keep the current regimen of immunomodulatory therapy (IMT). They were asked to reschedule their appointments after 4–8 weeks.
Patients were explained that they are a ‘group at risk’ due to IMT and that frequent clinic visits need to be avoided. Patients were, however, discouraged from abruptly discontinuing their IMT, including biologic agents, as discontinuation of some biologics can result in loss of response when treatments are reintroduced or even result in the formation of antibodies to the discontinued biologic.56
Urgent cases which require clinic visits are those having active posterior or panuveitis or active uveitic complications, such as inflammatory choroidal neovascular membrane or cystoid macular oedema. The aims of these visits are first to assess and treat the sight-threatening uveitic conditions or complications, and second to provide patients with a long-term treatment protocol.
The utilisation of state-of-the art imaging modalities such as the swept source OCT and the wide-field Optos fundus camera enabled complete and accurate documentation of the posterior segment findings. Thereafter, a treatment plan was developed after assessment in the uveitis service. While telemedicine in vitreoretinal diseases has shown an increase in cost-effective means in screening for DR, ROP and age-related macular degeneration,57 previous publications on uveitis revealed that diagnosis based solely on fundus photographs and fluorescein angiogram images performed poorly, and supported a recommendation against using fundus images alone to determine diagnosis in uveitis.58
Optometry service
SARS-CoV-2 has been reported to be potentially transmitted through the mucous membranes of the eye59 and enters the tears through droplets, which may pass through the nasolacrimal ducts and into the respiratory tract.60 These facts rose concerns with respect to fitting contact lenses and using trial sets particularly if the virus remains on the surface of the lens, even for several days. In order to minimise the risk of staff and patient infection, the contact lens and refraction clinics were closed, except biometry tests for urgent surgeries.
Cataract service
Non-urgent elective cataract clinic and cataract operations were suspended in order to reduce the risk of disease transmission.5 Cancellation of non-urgent cataract surgeries can reduce the risk of viral transmission,61 outweighing the surgical benefits of cataract operation. Emergency cataract surgeries are indicated in cases of phacomorphic glaucoma, phacolytic glaucoma and penetrating ocular trauma.1 62 63
Telemedicine may be used to follow up patients who underwent cataract surgery.47 This follow-up method enabled us to monitor postoperative recovery and identify complications as early as possible. The patients are not examined 1 week postoperation or 1 month postoperation, as they used to pre-corona days, and are guided via telephone about postoperation management, mainly the usage of topical eye-drops. Visual acuity is assessed by asking the patient to evaluate their vision by performing daily tasks, such as the ability to read subtitles on a television screen.
Glaucoma service
Glaucoma service was divided into three divisions: intervention, screening and monitoring patients. Intraocular pressure (IOP)-lowering modalities necessitate physical presence of the patient in the treating centre. Due to the potential risk of infection by using reusable eye equipment such as the Goldmann applanation tonometer, interventions were confined only to urgent and emergent cases, including primary and secondary acute angle-closure glaucoma, and primary and secondary open-angle glaucoma with uncontrolled IOP that is sight-threatening.64 65 For screening and monitoring purposes, parameters were taken into consideration in assessing glaucoma, including IOP, corneal thickness, anterior chamber depth and morphology, optic disc appearance, retinal nerve fiber layer (RNFL) thickness, and the current visual field map. To minimise interactions, these parameters were measured remotely, by trained technicians, and sent to the treating physician, skipping patient–physician encounters.
Teleglaucoma is used to follow up non-urgent cases with instructions about treatment especially for IOP-lowering therapy.66 The diagnosis and management of glaucoma are significantly associated with IOP, but contemporary office-based measurements are not enough to discover diurnal changes and spikes, nor do they demonstrate the effect of medication and compliance. Therefore, patient-directed self-tonometry can be taken throughout the day and is becoming an important part of the delivery of care to patients with glaucoma. Potentially, a secure central database that automatically flags IOPs and alerts the treating ophthalmologist electronically can be used. This provides marked benefit to patients who live remotely from their treating ophthalmologist and may be useful for population screening programmes.67 68
Ocular oncology service
A recent study from Guangzhou, China69 showed that patients with cancer are at a higher risk of developing severe events in COVID-19, with an HR of 3.56. Therefore, some oncologists suggested considering postponing adjuvant chemotherapy or elective surgery for less aggressive cancers. In contrast, it is well established that delayed oncological surgery may lead to disease progressions and result in tumours no longer resectable, leading to worse survival outcomes. Cortiula and colleagues70 stated that patients with advanced disease and no suggestive symptoms of COVID-19 should keep receiving planned chemotherapy or radiotherapy treatment, without unnecessary delays. Moreover, they highlighted that although postponing follow-up and cancer prevention appointments is a strategy to be considered, an excessive accumulation of visits or examinations risks burdening the national public health system over the next few months. Therefore, our ocular oncology service remained open for new patients with suspected ocular malignancies and follow-up of patients with known malignancies. The operating room was open to treat these patients, and specifically for examinations under anaesthesia and treatment of children with retinoblastoma. On the other hand, appointments of patients who were followed for nevi for an extended period have been postponed.
Treatments of ocular malignancies do not affect patients’ immune system and should not put them at risk for COVID-19. The exception is children with active retinoblastoma requiring intra-arterial chemotherapy as it has been known to cause neutropaenia in 1.2%–37.9% of patients.71 72
Similar with other indications for anti-VEGF therapy, patients with irradiation retinopathy continued to be treated during the SARS-CoV-2 outbreak.
Oculoplastic service
After an initial triage by telephone, non-urgent cases were given the option to undergo a telemedicine consultation or to delay their visit.6 Patients were also given the option to email a preliminary photo of their eyelid lesion, blood test results, eyelid malposition and all other relevant documentation prior to the consultation. Secured live media calls through applications73 or other media options were done as an alternative. Consultations with other subspecialties as well as multidisciplinary clinics were done using online applications.
Oculoplastic consultants were divided into two separate groups, each working on alternate days. A senior oculoplastic consultant examined all elective patients in clinic. Visual acuity tests were not done routinely and when indicated they were performed by the examining physician. Although the nasopharynx viral loads of COVID-19 have been reported to be lower than those found in the oropharynx, we elected to minimise our endoscopic examinations to emergencies only.74 All elective surgeries with no life-threatening or sight-threatening concerns were delayed.
Conclusions
With the evolving COVID-19 pandemic, and with its high infectivity that threatens health workers, crucial measures were adopted to reduce the risk of infection among eye care providers and patients, while saving their vision remains our priority.
Following recommendations and guidelines from several formal ophthalmology associations and the experience of other colleagues, a practice protocol was established to help overcome the ordeal with minimal unfavourable consequences. The benefits of these rearrangements remain to be proven.
References
Footnotes
Contributors JL planned the review, is responsible for the overall content and submitted the review. KS wrote the introduction, methods and conclusions, and is responsible for the overall content of the review. IC wrote the abstract. JK wrote the section on neuro-ophthalmology service. IA and HM wrote the section on paediatric ophthalmology service. AS, IL and DL wrote the section on cornea service. HA wrote the section on telemedicine. RA wrote the section on uveitis service. TJ wrote the section on retina service. HBE wrote the section on optometry service. SF wrote the section on ocular oncology service. LT wrote the section on imaging. GG wrote the section on glaucoma service. SO wrote the section on oculoplastic service. TLV wrote the section on cataract service.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement No data are available.