Article Text

Abstract
Objective To report the results of a global survey on cataract practice patterns related to preoperative, intraoperative and postoperative care, surgical setting and personnel allocation.
Methods and analysis An online 28 questions survey was sent to 240 ophthalmologists asking to describe prevailing trends in their institutions across 38 countries and 5 continents. Questions inquired country, institution, surgical volume and setting, anaesthesia, preoperative and intraoperative examination and postsurgical care. Statistical analysis used crosstabs lambda statistics for non-parametric nominal variables. P value less than 0.05 was considered statistically significant.
Results 209/240 (87%) ophthalmologists responded: 38% representing public hospitals, 36% private practices and 26% academic sites; overall surgical volume was between 241 700 and 410 500 cataracts per year. There was a significant correlation between type of institution and surgical volume. Complete results available in online (https://freeonlinesurveys.com/r/W6BcLLxy).
Conclusion Cataract surgery related patterns of perioperative care showed significant difference among respondents, regardless to type of institution, surgical volume and country. Many evidence-based procedures are unevenly practiced around the world and some widespread and expensive habits lack solid scientific evidence while consuming enormous amount of resources both monetary and human. There is a need to reach consensus and share evidence-based practice patterns.
- public health
- epidemiology
- treatment surgery
- lens and zonules
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of the study
What is already known about this subject?
Cataract surgery is a highly standardised surgical procedure with excellent results.
What are the new findings?
Perioperative procedures before and after surgery greatly vary among different surgeons and institutions and this may account for millions of euros of possibly unnecessary excess expenditures worldwide.
How might these results change the focus of research or clinical practice?
Standardising perioperative procedures can improve patients’ safety and possibly spare millions of euros and thousands of possibly unnecessary diagnostic procedures.
Introduction
Cataract extraction is the most prevalent surgical procedure of all medical specialties with an estimated 3.7 million cases per year in the USA, 7 million in Europe and 20 million worldwide.1 2
Phacoemulsification with intraocular lens implant in the capsular bag is the standard of care, resulting in excellent anatomic and functional outcome and relatively low complication rate.3 Although the surgical procedure is very consistently performed worldwide, practice patterns related to patients’ preoperative and postoperative care, diagnostics, surgical setting, precautions and follow-up, greatly differ, according to countless variables including institutions and country regulations, insurance company requirements, payment agreements and even surgeons’ preferences and habits.4
Given the exceedingly high volume of cataract procedures worldwide, perioperative setting and organisation are at least as important as the technical quality of surgery itself, due to their impact on patients’ rehabilitation, satisfaction, healthcare organisation, expenditures as well as on the medico-legal burden. Defining and validating a golden standard of ‘perioperative’ care, diagnostics and surgical theatre setting, would greatly help deliver homogeneous, evidence-based healthcare services throughout the world. Even more importantly, this would increase appropriateness and efficiency while improving the management of risk inherent to surgical procedures, reducing the medico-legal burden and freeing a significant amount of resources.
Purpose of present paper is to report the results of a worldwide online survey conducted to highlight the preferred patterns of practice related to preoperative, intraoperative and postoperative setting and organisation around cataract surgery. The survey, far from being ‘omni-comprehensive’, is intended to offer a glimpse on shared practices as well as notable distinctions in order to ignite discussion on the need for shared and validated procedures.
Materials and methods
Survey rationale and diffusion
An online survey consisting of 28 multiple choice questions reported in box 1 was sent to 240 leading ophthalmologists working in 240 different centres in 38 countries and five continents. All participants were contacted via email and previously instructed. Participants were recruited by the authors among colleagues previously contacted and willing to participate and also through a word-of-mouth mechanism. The Italian and Japanese Ophthalmological Society posted a call for participants to the survey thus enrolling more ophthalmologists than from any other participating country. The survey took approximately 20 min to complete and participants received no compensation.
Survey questions
Question
1. Please enter the state where your institution is located.
2. Type of institution.
Private practice.
Academic.
Public hospital NHS.
3. How many cataract surgeries per year are performed in your institution?
<500 per year.
Between 500 and 1000 per year.
Between 1000 and 2000 per year.
Over 2000 per year.
4. How many ophthalmic surgeons (MDs) are present at the same time in the OR during cataract surgery?
Only one, the surgeon.
Two surgeons.
One surgeon and one resident.
5. How many nurses are present at the same in the OR during cataract surgery?
No nurses, the surgeon is alone.
One circulating nurse.
One scrub nurse.
One scrub and one circulating nurse.
Resident/fellow as a scrub nurse alone.
Resident/fellow and a circulating nurse.
6. Type of anaesthesia for uncomplicated routine cases.
>90% topical.
75% topical 25% peribulbar.
50% topical 50% peribulbar.
10% topical 90% peribulbar
7. Is there an anaesthesiologist?
Dedicated MD present in the OR during all surgery.
Dedicated nurse anaesthesiologist present in the OR during all surgery.
MD available for sedation on demand in the operating group.
MD available only for emergency.
8. Sedation.
None >90%.
Benzodiazepines >90% of cases.
Benzodiazepine 50% of cases.
Benzodiazepine 25% of cases.
Opioids >75% of cases.
Opioids 50% of cases.
Opioids 25% of cases.
9. Does the patient have a vascular access during routine cataract surgery?
100% of patients.
Only if deemed necessary: about 75%.
Only of deemed necessary: about 50%.
Only if deemed necessary: about 25%.
Never.
10. Does the patient have continuous ECG monitoring during routine cataract surgery?
100% of cases.
No, never.
Only in deemed necessary, roughly 75% of cases.
Only if deemed necessary, roughly 50% of cases.
Only in deemed necessary, roughly 25% of cases.
Only in deemed necessary, roughly 5% of cases.
11. Does the patient have continuous blood pressure monitoring during routine cataract surgery?
100% of cases.
No, never.
Only in deemed necessary, roughly 75% of cases.
Only if deemed necessary, roughly 50% of cases.
Only in deemed necessary, roughly 25% of cases.
Only in deemed necessary, roughly 5% of cases.
12. Pre-op ocular diagnostics ROUTINELY used.
Optic biometry.
Ultrasound biometry.
Endothelial microscopy.
Corneal topography.
Macular OCT.
Potential Acuity Meter.
13. Preoperative testing.
Topical antibiotics.
No pre-op therapy.
Topical NSAIDs.
Topical antiseptics.
Sistemic antibiotics.
14. Use of anticoagulants/antiaggregants.
Leave as it is.
Discontinue before surgery.
Substitute with LMW heparin.
Ask patient’s GP.
15. Preoperative prophylaxis.
Topical antibiotics.
No pre-op therapy.
Topical NSAIDs.
Topical antiseptics.
Sistemic antibiotics.
16. Povidone iodine before surgery.
100% of cases.
Most cases.
Never.
17. Intra-op endophthalmitis prophylaxis at the end of surgery.
No prophylaxis.
Intracamerular cefuroxime.
Other intracamerular drug.
Conjunctival sac povidone iodine.
Conjunctival antibiotics.
18. Mark all materials changed with a sterile one after EACH and EVERY routine cataract surgery.
Pump cassette.
All tubings.
Phaco handpiece.
Phaco tip.
BSS bottle.
Phaco tray draping.
19. Management of intraoperative systemic pressure spikes/anxiety.
Surgeon prescribes drugs.
Anaesthesiologist prescribes drugs.
Nurse administers drugs based on predetermined protocol.
20. Post-op patching.
None.
For a few hours.
At night for few days.
For a few days H24.
21. Post-op restrictions.
None.
No social activities/work 5 days.
No social activities/work 12 days.
No social activities/work >15 days.
22. Post-op therapy.
None.
Topical antibiotics+topical NSAIDs.
Topical NSAIDs alone.
Topical antibiotics alone.
Systemic antibiotics+topical.
23. Second eye.
At patient’s will.
Same day.
Within 7 days.
Within 15 days.
Within a month.
Within 3 months.
24. Length of stay within the premises of the Surgical Centre AFTER surgery for monitoring reason.
Few minutes.
At least 1 hour.
At least 2 hours.
At least 3 hours.
25. Who discharges the patient from surgical centre after surgery?
The surgeon.
A nurse based on surgeon written order.
A second ophthalmologist.
The patient is free to leave whenever comfortable.
26. Post-op visit schedule is approximately.
Days 1, 7, 30.
Days 7, 30.
Day 30.
27. Who sees the patient post routine cataract surgery?
Always same surgeon.
Any ophthalmologist on duty in the day of control visit.
Referring ophthalmologist.
Optometrist.
Nurse.
28. If cost were NOT an issue would you like a dedicated anaesthesiologist?
Not necessary.
Yes.
Available for sedation in the same floor is enough.
Available only for emergency is enough.
BSS, Balancend Salt Solution; GP, General Practitioner; LMW, Low Molecular Weight; NHS, National Health System; NSAIDs, non-steroid anti-inflammatory drugs; OCT, Ocular Coherence Tomography; OR, operating room.
Rationale behind questions was as follows: questions 1–3 described country of origin, type of institution and surgical volume. Questions 4–11 described the surgical theatre setting, number of ophthalmologists, nurses, anaesthesiologists, type of anaesthesia, safety precautions including venous access, continuous ECG and pressure monitoring.
Questions 12–19 evaluated preoperative diagnostics, infection prophylaxis and intraoperative material sterility and systemic management while questions 20–27 dealt with postsurgical care: patching, discharging and second eye surgery. The very last question touched one of the sensitive issues: whether the presence of an anaesthesiologist would be always desirable if cost were not an issue.
Data were gathered in .xls format for analysis and statistical purposes.
The survey was administered in English language and all participants were fluent in English. Question and answers are publicly available in online and online supplemental file (survey results final.pdf).
Supplemental material
Patients were not involved in the study as practice patterns was the object.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors and there are no competing interests to be disclosed.
Statistical analysis
Statistical analysis used Cramer-V and symmetric Lambda statistics of contingency tables on nominal variables. Multilevel structural equation modelling determined the difference between the surgical theatre setting with staff employed and the preoperative, intraoperative and postoperative diagnostics and prophylaxis in the five continents. P values less than 0.05 have been considered statistically significant.
Results
The complete survey results are public and accessible online at the above URL. Overall response rate was 209/240 (87.08%) from 38 countries (figure 1). The survey represented all types and sizes of institutions: 38% public hospitals, 36% private practices and 26% academic sites; 40% of them with a surgical volume greater than 2000 and 40% between 1000 and 2000 per year for overall surgical volume between 241 700 and 410 500 cataracts per year. There was a significant correlation between type of institution and surgical volume (p<0.05): public hospitals had larger surgical volume.
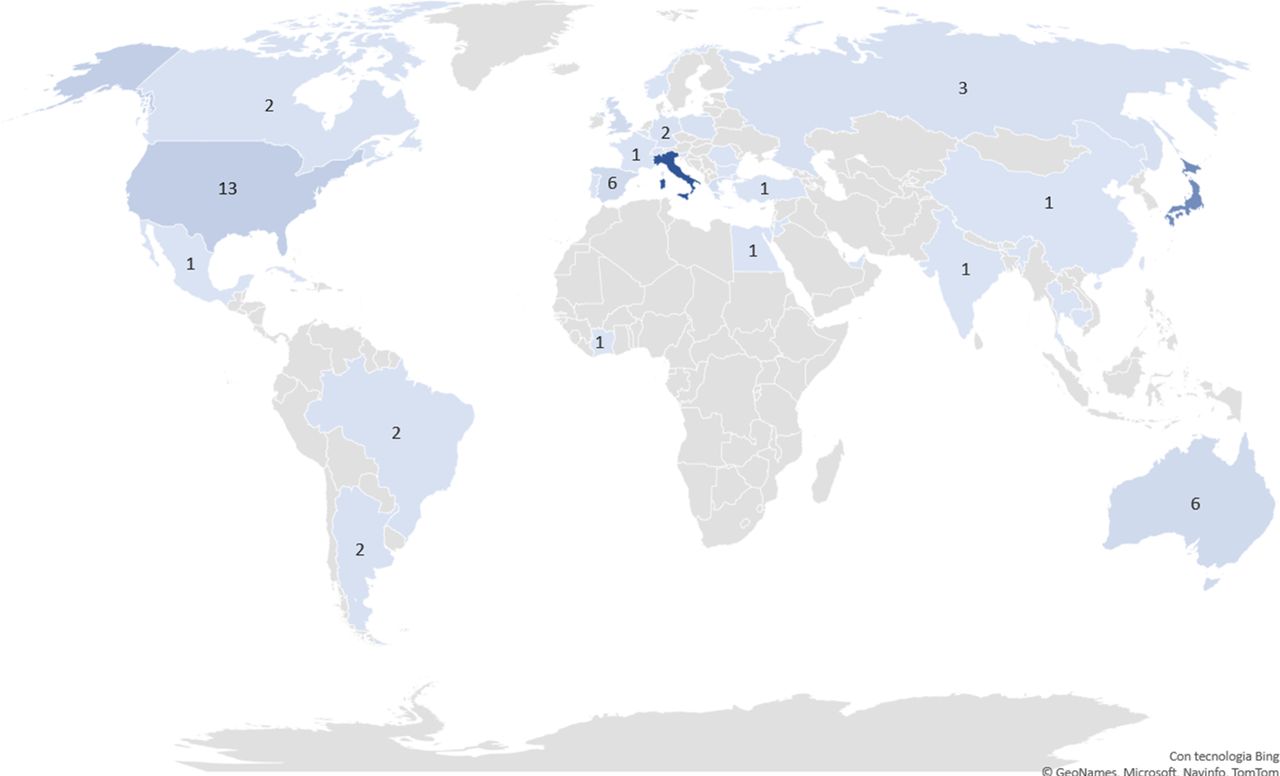
Survey geographic coverage. All countries in blue had one respondent except countries where the number of respondents is reported on the map. Italy had 83 responders and Japan 51.
Preoperative systemic testing varied considerably among respondents (figure 2): 52% of involved institutions had mandatory preoperative ECG and blood testing, in 126/209 (60%) centres was the ophthalmologist who interviewed patient on his/her systemic conditions while in 57/209 institutions an anaesthesiologist briefed the patient. In such all such cases, patients also underwent ECG and blood tests. Interestingly, 13/203 centres (6%) did not ask for any pre-op testing, neither interviewed the patient, while 65/209 (31%) required the patient to fill a questionnaire and 34/209 (16%) had the general practitioner doing it. Neither institution type nor surgical volume had an impact on systemic pre-op testing (table 1).

Systemic testing routinely performed for each cataract surgery by responders. Note percentages add up to more than 100% since multiple answers were allowed.
Survey questions when type of institution and surgical volume are considered independent variables
Antiplatelet aggregation drugs and anticoagulants were left untouched in 75% of cases and discontinued in 12% while pre-op topical prophylaxis was performed in 71% of interviewed institutions while the remainder 29% did not. Fifty-four per cent or responders used antibiotics, 29% non-steroid anti-inflammatory drugs (NSAIDs), 29% antiseptics and multiple choices were common: 6.9% used three products; 21% two drugs, 68% only one drug. Institutions requiring one drug only prescribed: 61/85 (71.7%) antibiotics, 15/85 (17.6%) antiseptic drugs alone, 9/85 (10.6%) NSAIDs (figure 3).

Number of drugs routinely prescribed as pre-op prophylaxis.
Preoperative ocular diagnostics varied considerably (figure 4): 87% performed optic biometry, 28% ultrasonic biometry, 55% endothelial microscopy, 47% Optical Coherence Tomography (OCT), 30% corneal topography. Interestingly, 26/209 (12.4%) performed ultrasonic biometry as the only pre-op diagnostics; 2.9% of responders performed all six tests, 7.8% performed five tests, 13.3% four tests, 27.5% three tests, 29.5% two tests and 18.7% only one test. Institution type but not surgical volume significantly influenced this choice: 38% of private practices performed four or more tests versus 20% academic centres and 11% of public hospitals (table 1).
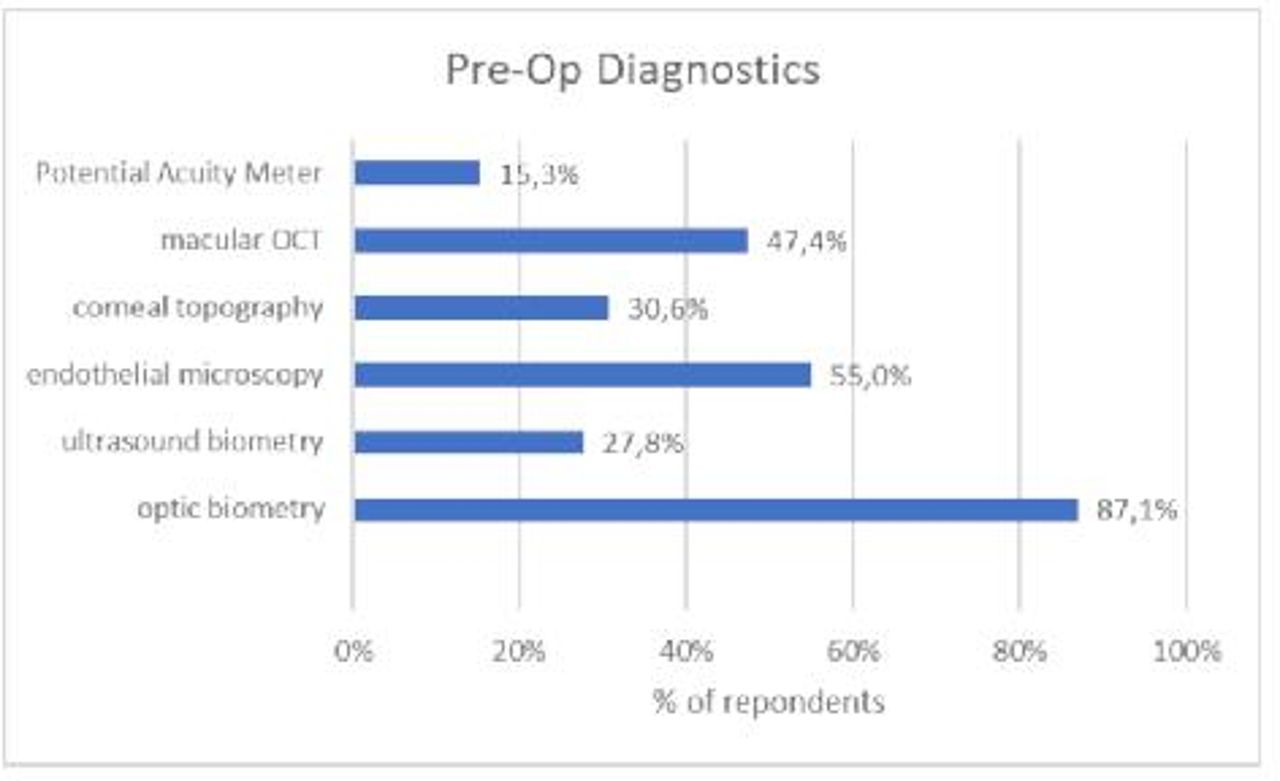
Ocular diagnostics routinely performed for each cataract surgery by responders. Note percentages add up to more than 100% since multiple answers were allowed.
Surgeon was alone in the operating room (OR) in 45% of cases, assisted by a resident in 29% or second house-staff surgeon in 26%; the type of institution significantly influenced the number of surgeons (table 1): private practitioners were more likely to operate alone (74% of centres vs 13% academic and 42% public hospitals) while the surgical volume did not correlate to the number of surgeons present in the OR.
Two nurses (one scrub and one circulating) were present in 78% of cases, only one circulating nurse in 11%. A dedicated anaesthesiologist was present in the OR throughout surgery only in 30% of cases, available for sedation in 29% or on call within the premises of the hospital for emergency only, in 31% while 10% relied on a nurse anaesthesiologist (a professional that does not exist in many countries) although if cost were not an issue, 51% of responders would like a dedicated anaesthesiologist (see complete results online). Type of institution but not surgical volume (table 1) influenced significantly the wish for a dedicated anaesthesiologist: 24% of private practices, 20% of academics and 7% of hospitals felt it was not necessary while respectively 47%, 39% and 60% disagreed.
Topical anaesthesia was used in more than 90% routine, uncomplicated cases in 81% of responding centres. Sixty-nine per cent of respondents used no sedation in over 90% of their cases, while 15% used benzodiazepines in over 90% of their patients and 10% only in 50%. The presence of a dedicated anaesthesiologist influenced the use of sedation (λ 0.08; p=0.004) but not the type of anaesthesia or the amount of preoperative systemic testing.
A vascular access was routinely placed in 60% of centres (type of institution influenced significantly vascular access, being more frequent in public hospitals: 76% versus 64% in academic centres and 40% of private practices; p<0.01; table 1). Sixty-nine per cent of responders placed continuous ECG monitoring and 81% pressure monitoring.
The use of povidone iodine before surgery was 95% while at the end of surgery 59% injected cefuroxime in the anterior chamber (AC), 12% injected other drugs in the AC, 34% instilled povidone in the conjunctival sac, 23% antibiotics and 13% did not use any drug at all.
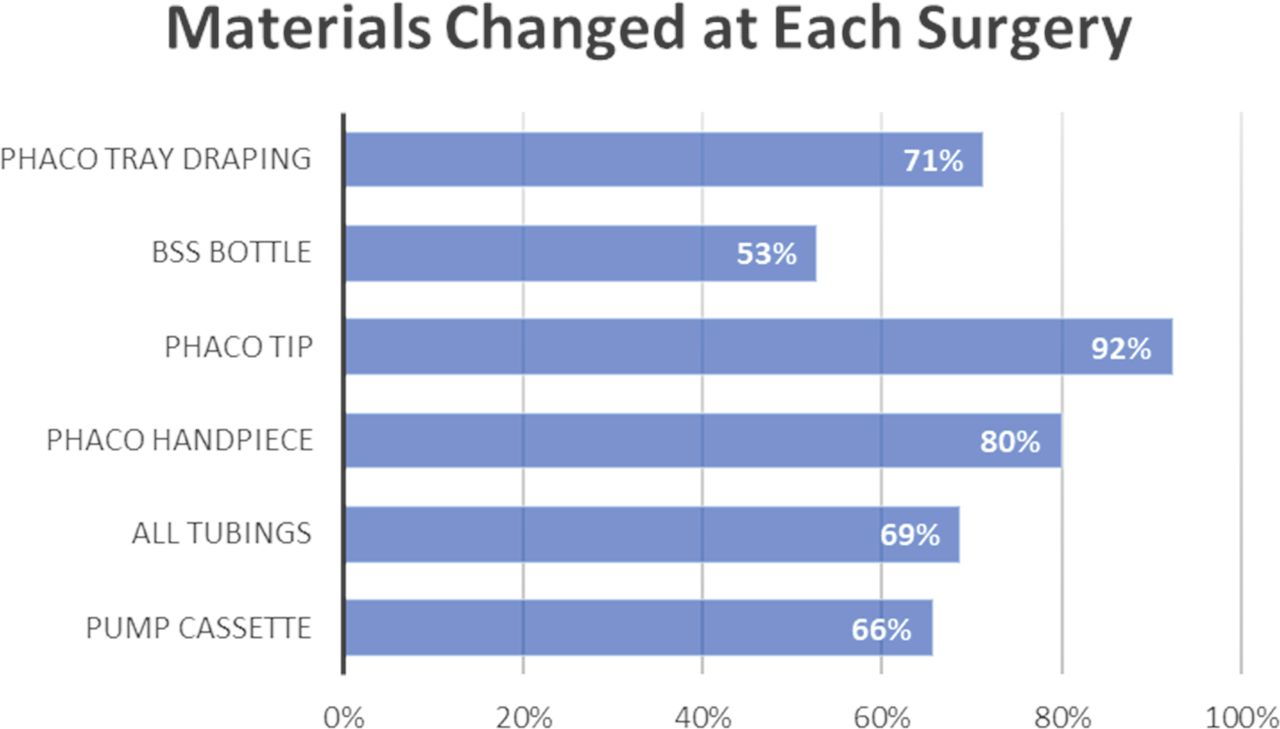
Surgical material sterility management and the exchange of used materials after every single procedure showed great variability (figure 5): 92% changed the phaco tip, 80% the handpiece, 71% phaco tray draping, 69% the entire tubing set and only 53% all six items. Type of institution significantly impacted on this issue: 30% of private practices, 71% of academic centres and 87% of hospitals changed five or more materials after each and every surgery (table 1).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sterility management: materials changed every single surgery. Note percentages add up to more than 100% since multiple answers were allowed.
Postoperative care was administered as follows: patients were discharged from surgical centre after at least an hour in 49% of cases, a few minutes after surgery in 36% mostly by a nurse on written orders by the surgeon (59%) or by the surgeon him/herself (15%) with topical antibiotics and anti-inflammatory drugs in 89% or responses with a return visit schedule of 1, 7, 30 days in 87% of cases, done by the surgeon in 40% of cases and any ophthalmologist on duty in 53% of cases. Patching was ordered for a few hours in 48% of cases, at night for a few days in 25% of responses while 23% did not recommend any patching. Restrictions also varied: 51% precluded social activity and work for 5 days while 43% did not recommend any. Postoperative care is influenced by institution type but not surgical volume (table 1).
Second eye surgery schedule ranged from 7 days to 3 months with most centres allowing the patients to decide anytime (33%). Only 5% scheduled same day bilateral surgery.
Discussion
Cataract surgery is the most prevalent surgery of all medical fields, very consistently performed throughout the world with high rehabilitation rate. While the surgical technique is extremely standardised, preoperative, intraoperative and postoperative procedures greatly vary according to surgeons’ preferences, institution and country regulations.5
Our survey represents a snapshot of this extremely variegated scenario: despite the existence of guidelines6 7 and scientific evidence, there seems to be little consensus on many key issues, strengthening the need for the definition of a ‘best practice’, given the gigantic caseload, the number of stakeholders and the economic and medico-legal implications.8
Although the questionnaire topics regarded numerous aspects of cataract surgery process, our discussion will focus on costs and safety.
A single surgeon is present in 40% of ORs and 30% use a resident as second surgeon; there is a dedicated anaesthesiologist only in 30% of cases, while is available for sedation on demand in 29% and reachable only for emergency in another 31%. Two nurses are present in 77% of ORs.
The copresence of two surgeons, mandatory in some countries (eg, Italy) and recommended in other specialties,9 may questionably increase safety and certainly cost: assuming a 20 min uncomplicated surgery, medical staff cost per surgery varies from US$46 for a single surgeon and available anaesthesiologist, to US$120 for two surgeons and a dedicated anaesthesiologist (table 2), translating into 1.2 million physician hours or 132 million dollars in the USA (assuming US$110 average cost per hour) and about twice as much in Europe! It all doubles for a dedicated anaesthesiologist.
Perioperative practice patterns and projected costs
Intraoperative monitoring also returns inconsistent data: vascular access is routinely placed only in 60% of centres, ECG in 69%, ECG and continuous pressure measurement in 81%. There clearly is a need for a univocal recommendation in the interest of safety although venous access itself can be a matter of controversy as oral sedation has been proved to be at least as effective as intravenous10 and accurate patient selection could limit its use to those more likely to require pharmacological treatment. In any case, a vascular access has very limited impact on cost but is potentially life-saving and continuous monitoring of a patient with no vascular access is almost of no use since intravenous drugs cannot be quickly administered on need.
The amount of preoperative ocular diagnostics is even more variable: 40% do four or more tests and 20% only one. The difference of cost and healthcare personnel time is striking: assuming an average US$35 per each diagnostic test, the delta between a single biometry test (mandatory) and the entire panel of six mentioned tests, is US$175 per surgery or 647 million in the USA and twice as much in Europe without even considering medical staff adjunctive time costs that certainly exceed 1 hour per surgery (another US$110 per surgery).
Routine preoperative medical tests requested by 50% of survey responders have been often alleged unnecessary11–13 and replaced with preoperative assessment by a physician with or without the help of self-administered questionnaires14 as was the case in our survey. It should be noted that both raise direct and indirect costs: a basic panel of blood exams has an average cost of US$25 and ECG US$30 (US$55 per surgery) plus at least 30 min of personnel time adding another US$55 per procedure,15 while physical assessment and interview would require at least 20 min of a physician (US$110/3=US$36.6 per surgery). A summary of cost and scientific support for the most sensitive issues touched by our survey is reported in table 2.
Anaesthesiologists raise multiple issues: safety, costs and also comfort: while only 30% of interviewed surgeons have a dedicated one, 51% would like one and form the patients’ perspective, the possibility of some form of sedation is certainly desirable. Indications for sedation represent a key issue with regard to the presence of an anaesthesiologist: for some patients (and surgeons) sedation is just a ‘plus’ to live better the surgical experience16 while in other cases a good sedation makes the difference between being able to perform surgery without complications or not.
Provided safety is guaranteed, institutions may decide differently: a private practice may wish to offer sedation for a better ‘surgical experience’ and attract anxious patients while high volume hospitals may elect to use a single anaesthesiologist to cover multiple contiguous ORs at the same time.
Preoperative prophylaxis is another area of variability: 54% use topical antibiotics despite most literature proving this does not reduce either intraoperative ocular surface bacterial count17 or the risk of endophthalmitis18 19 especially if cefuroxime20 or moxifloxacin21 is administered in the AC at the end of surgery. This issue has several implications: while patients’ safety does not seem to improve, drug cost (assuming US$20 per vial)22 is 74 million dollars in the USA (and 140 million in Europe) with the only potential effect of increasing bacterial resistance.
NSAIDs improve mydriasis23 and reduce inflammation24 while their prophylactic role in preventing cystoid macular oedema is controversial and has been demonstrated only in diabetic patients.25 26 About one-third (28%) of survey responders use them routinely (table 2) accepting a further cost of roughly US$20 per surgery.
Endophthalmitis prophylaxis relies on two documented cornerstones well represented in our survey: conjunctival sac povidone iodine 5% before surgery27 (95% of responders do it routinely) and intracamerular antibiotic2 (71%). It is surprising that 29% do not use intracamerular antibiotics despite the existence of data from a well-designed multicentre study28 and evidence on other molecules29 30 allowing a drastic endophthalmitis risk reduction at low cost (table 2).
Surgical materials exchange after each and every surgery also yielded surprising responses: 92% change phaco tip, 80% handpiece, 71% phaco tray draping, 69% all tubing, 66% pump cassette and 53% Balanced Salt Solution (BSS) bottle. These results raise concern since there is no question that the first four issues contaminate during surgery31 and most likely even the cassette and BSS bottle despite filters, valves and a pressure gradient. Recommend exchanging all phaco materials with disposable sterile pack, as indicated by manufacturers forbidding a second use, costs about US$7032 and has an obvious impact on safety at a reasonable cost. Reusable or partially reusable tubing and cassettes allow a reduction of costs adding some sterility expenses.
Postsurgery patient management also yielded somewhat contrasting results with minimal or no impact on costs and uncertain effect on safety: 36% dismiss patients a few minutes after surgery while 64% keep them for at least an hour; 43% do not limit social activities in any way while 51% do so for 5 days.
Regardless to institutions and countries, survey results suggest the following practice pattern as the most prevalent although with notable distinctions: half patients undergo blood testing and ECG, virtually all are instructed to keep their antiplatelet aggregation drugs and more than half receive preoperative antibiotic topical prophylaxis. Povidone iodine and intra-cameral cefuroxime endophthalmitis prophylaxis are very widespread while surgery is mostly performed by a single surgeon sometimes assisted by training doctor, one scrub and one circulating nurse, under topical anaesthesia with an anaesthesiologist on call for emergency only. Only the phaco tip is changed for every surgery in most cases and a vascular access is obtained in 60% of patients with continuous ECG monitoring and brachial pressure monitoring in 70%.
Our results clearly indicate an overall global inconsistency of most cataract practices deeply impacting costs and most likely generating diverse levels of patients’ security. It is surprising that surgical volume did not impact significantly in any inquired matter, as opposed to institution type, in other words hospital, academic and private practices do not seem to converge to an overlapping workflow organisation even when dealing with comparable surgical volumes as if it were impossible (or there if were no interest) in establishing a shared ‘best practice’ (table 1).
Given the exceedingly high number of patients involved, reaching consensus on validated and shared golden standard seems advantageous if not mandatory and would produce a manifold impact on healthcare: improve safety, rationalise cost and free consistent monetary and human resources.
The limitations of present study are numerous and include the unequal response rate from different Countries and the extremely limited number of responders per country, in many instances only one. Nonetheless responses cover a vast number of surgical procedures well distributed among all types of institutions and the wide variability of reported behaviours is indeed the most interesting result and could only have increased with more responders. We therefore believe those pitfalls scarcely impact what is regarded as the main outcome: disclose an extreme practice variability.
Scientific and professional societies hold the responsibility for deploying evidence-based standard of care and encourage consistent, diffuse application. An international committee promoted by large scientific societies would be desirable.
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TR, MRR and DI designed the study and wrote the manuscript. LG, VR, ID and GR revised data, run statistics and proofread the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.