Article Text

Abstract
Aim To assess the clinical outcomes following the use of toric implantable collamer lenses (toric ICL, STAAR Surgical) for the correction of high myopic astigmatism with keratoconus.
Methods This retrospective study evaluated 21 eyes of 11 patients with spherical equivalents of −9.70±2.33 D (mean±SD) and astigmatism of −3.21±1.56 D who underwent toric ICL implantation for keratoconus. Preoperatively, and at 1, 3 and 6 months and 1, 2 and 3 years postoperatively, we assessed the safety, efficacy, predictability, stability and adverse events of the surgery.
Results The logarithm of the minimum angle of resolution (logMAR) uncorrected distance visual acuity (UDVA) and the logMAR corrected distance visual acuity (CDVA) were −0.06±0.11 and −0.12±0.09, respectively, at 3 years postoperatively. At 3 years, 67% and 86% of the eyes were within ±0.5 and ±1.0 D, respectively, of the targeted correction. Manifest refraction changes of 0.04±0.33 D occurred from 1 month to 3 years postoperatively. No significant change in manifest refraction (analysis of variance, p=0.989) or keratometry (p=0.951), or vision-threatening complications occurred during the observation period.
Conclusions Toric ICL implantation is beneficial according to measures of safety, efficacy, predictability and stability for the correction of refractive errors for keratoconus during a 3-year observation period. The disease did not progress even in the late-postoperative period, suggesting the viability of this procedure as a surgical option for the treatment of such eyes.
- Treatment Surgery
Statistics from Altmetric.com
Introduction
Keratoconus is a progressive non-inflammatory disorder characterised by the progressive thinning and subsequent anterior protrusion of the cornea causing both severe myopic astigmatism and asymmetrical irregular astigmatism. Treatment for keratoconus varies with stage, but the first choice is frequently the use of a rigid gas-permeable contact lens. However, in eyes with an irregularly shaped cornea or allergic conjunctivitis, contact lens intolerance may arise. The fact that diagnoses of keratoconus have been made in relatively large numbers (6.4–9.6%) of candidates unsuitable for refractive surgery1 ,2 suggests that patients with keratoconus seeking refractive surgical intervention are more numerous than expected.
The Visian Implantable Collamer Lens (ICL, STAAR Surgical, Nidau, Switzerland), a posterior chamber phakic intraocular lens (IOL), has received favourable reports both for its superior postoperative visual performance and for its better safety and greater effectiveness for the correction of moderate to high ametropia. Moreover, the toric ICL is known to be effective for the correction of moderate to high myopic astigmatism. Several reports have discussed toric and non-toric ICL implantation for the correction of refractive errors in patients with mild and stable keratoconus,3–14 and we have shown that toric ICL implantation gives good results as regards safety, efficacy, predictability and stability in the correction of high myopia throughout the 6-month follow-up period.7
Since corneal biomechanical parameters are reportedly already compromised in keratoconus,15–17 and since this surgical technique requires a 3.0–3.2 mm temporal corneal incision, the disease may progress in the late-postoperative period, resulting in distortion of the cornea and subsequent refractive errors in patients with keratoconus. Accordingly, it is clinically important to assess the long-term visual and refractive outcomes of toric ICL implantation for keratoconus, given the prevalence of this technique. We extended the study further in order to investigate the long-term (3-year) clinical outcomes of toric ICL implantation for the correction of refractive errors for mild and stable keratoconus in a multicentre study.
Patients and methods
Twenty-one eyes of 11 patients (four men and seven women) who underwent implantation of a posterior phakic implantable collamer lens (Visian ICL, STAAR Surgical) for the correction of moderate to high myopic astigmatism at four major medical institutions (Kitasato University Hospital, Sanno Hospital, Nagoya Eye Clinic and Nakamura Eye Clinic) and who regularly returned for postoperative examination and completed a 3-year follow-up, were included in this retrospective observational study. Some of the subjects have already been described in a previous report.7 The sample size in this study offered 83% statistical power at the 5% level in order to detect a 0.10 difference in the logarithm of the minimum angle of resolution (logMAR) of visual acuity, when the SD of the mean difference was 0.15. The inclusion criteria for this surgical technique for treating keratoconus in this study were as follows: a corrected distance visual acuity (CDVA) of 20/25 or better, a clear central cornea, an anterior chamber depth ≥2.8 mm, age ≥30 years and stable keratometry and refraction (no increase in corneal maximum keratometry (K2) greater than 1.0 dioptre (D) and no increase in cylinder greater than 0.5 D) for at least 1 year. The diagnosis of keratoconus was established by a combination of computed videokeratography, keratometric readings and corneal pachymetry. All eyes had grade I or II keratoconus according to the Amsler-Krumeich classification, based on astigmatism, corneal power, corneal transparency and corneal thickness. Eyes with pellucid marginal degeneration having inferior corneal thinning with ectasia above the area of thinning and no inflammatory signs on slit-lamp biomicroscopy were excluded from the study. Preoperatively, and at 1, 3 and 6 months and 1, 2 and 3 years postoperatively, we determined the following: logMAR of uncorrected distance visual acuity (UDVA), logMAR of CDVA, manifest refraction (spherical equivalent and refractive cylinder), intraocular pressure (IOP), mean keratometric readings, corneal astigmatism and endothelial cell density (preoperatively and 3 years postoperatively), in addition to performing the usual slit-lamp biomicroscopic and funduscopic examinations. Contact lens use was discontinued at least 1 month before the preoperative examination was carried out. Before surgery, the horizontal white-to-white distance and anterior chamber depth were measured using a scanning-slit topograph (Orbscan IIz, Bausch & Lomb, Rochester, NY, USA), and the mean keratometric readings and corneal astigmatism were measured using an autorefractometer (ARK-700A, Nidek, Gamagori, Japan). The IOP was assessed with a non-contact tonometer (KT-500, Kowa, Tokyo, Japan). The endothelial cell density was determined with a non-contact specular microscope (SP-8800, Konan, Nishinomiya, Japan). The surgically induced astigmatism was assessed by vector analysis (Holladay–Cravy–Koch formula) using the keratometric readings preoperatively and 3 months postoperatively. Written informed consent was obtained from all patients for the ICL surgery for keratoconus. This retrospective review of data was approved by the Institutional Review Board at Kitasato University and followed the tenets of the Declaration of Helsinki. Our Institutional Review Board waived the requirement for informed consent for this retrospective study.
Toric implantable collamer lens power calculation
Toric ICL power calculation was performed by the manufacturer (STAAR Surgical) using the astigmatism decomposition method. In all eyes, emmetropia was selected as the target refraction to reduce the preoperative refractive errors as much as possible. Toric ICLs were manufactured to minimise rotation from the horizontal meridian. The size of the ICL was also chosen by the manufacturer on the basis of the horizontal corneal diameter and anterior chamber depth determined with scanning-slit topography (Orbscan IIz).
Toric implantable collamer lens surgical procedure
Before surgery, the patients underwent two peripheral iridotomies with a neodymium-YAG laser. On the day of the procedure, the patients were administered dilating and cycloplegic agents. To control for potential cyclotorsion in a supine position, the zero horizontal axis was marked preoperatively using a slit-lamp. A Mendez ring was also used for intraoperatively measuring the required rotation from the horizontal axis. After topical anaesthesia, a model V4b toric ICL (without a central hole) was inserted through a 3 mm clear corneal incision with the use of an injector cartridge (STAAR Surgical) after placement of viscoelastic material (Opegan, Santen, Osaka, Japan) into the anterior chamber. After the ICL had been placed in the posterior chamber, the remaining viscoelastic material was completely washed out of the anterior chamber with balanced salt solution, and a miotic agent (acetylcholine chloride; Ovisort, Daiichi-Sankyo, Tokyo, Japan) was instilled. After surgery, steroidal (0.1% betamethasone; Rinderon, Shionogi, Osaka, Japan) and antibiotic (levofloxacin; Cravit, Santen, Osaka, Japan) medications were topically administered four times daily for 2 weeks, after which the frequency was steadily reduced.
Statistical analysis
All statistical analyses were performed using StatView V.5.0 (SAS, Cary, NC, USA). One-way analysis of variance (ANOVA) was used for the analysis of the time course of changes, with the Dunnett test for multiple comparisons. The Wilcoxon signed-rank test was used for statistical analysis to compare the pre- and post-surgical data. Unless otherwise indicated, the results are expressed as mean±SD, and a value of p<0.05 was considered statistically significant.
Results
Study population
Preoperative patient demographics are summarised in table 1. Patients at the time of surgery were aged 38.7±6.6 years (30–48 years). The preoperative manifest spherical equivalent and refractive cylinder were −9.70±2.33 D (−5.75 to −13.75 D) and −3.21±1.56 D (−1.00 to −6.00 D).
Patient demographics of the study population undergoing posterior chamber phakic intraocular lens implantation for keratoconus
Safety outcomes
LogMAR CDVA was −0.12±0.07, −0.13±0.08, −0.13±0.09, −0.13±0.10, −0.11±0.09 and −0.12±0.09 at 1, 3 and 6 months and 1, 2 and 3 years postoperatively, respectively (ANOVA, p=0.989). Six eyes (29%) showed no change in CDVA, nine eyes (43%) gained one line, two eyes (10%) gained two lines, four eyes (19%) lost one line, and no eyes lost two or more lines 3 years after toric ICL implantation (figure 1). The four eyes which lost one line possibly did so due to a slight increase in higher-order aberrations or mild macular atrophy, but they had a CDVA of 20/20 or more.

Changes in corrected distance visual acuity 3 years after toric posterior chamber phakic intraocular lens implantation in eyes with keratoconus. CDVA, corrected distance visual acuity.
Effectiveness outcomes
LogMAR UDVA was −0.04±0.16, −0.06±0.16, −0.06±0.17, −0.04±0.17, −0.06±0.12 and −0.06±0.11 at 1, 3, and 6 months and 1, 2 and 3 years postoperatively, respectively (ANOVA, p=0.995). At 1, 3 and 6 months and 1, 2 and 3 years postoperatively, 95%, 95%, 100%, 100%, 100% and 100% of eyes, and 76%, 81%, 71%, 71%, 71% and 71% of eyes had a UDVA of 20/40 and of 20/20 or better, respectively (figure 2).

Cumulative percentages of eyes attaining specified cumulative levels of uncorrected distance visual acuity (UDVA) 3 years after toric posterior chamber phakic intraocular lens implantation in eyes with keratoconus. CDVA, corrected distance visual acuity.
Predictability
A scatter plot of the attempted versus the achieved correction (spherical equivalent) is shown in figure 3. At 3 years postoperatively, 67% and 86% of eyes were within ±0.5 and ±1.0 D of the attempted spherical equivalent correction, respectively. At 3 years postoperatively, 52% and 76% of eyes were within ±0.5 and ±1.0 D of the attempted astigmatic correction, respectively (figure 4).

A scatter plot of the attempted versus the achieved manifest spherical equivalent correction 3 years after toric posterior chamber phakic intraocular lens implantation in eyes with keratoconus.

Percentages of eyes within different dioptre ranges of the attempted correction (spherical equivalent) 3 years after toric posterior chamber phakic intraocular lens implantation in eyes with keratoconus.
Stability
Spherical equivalent
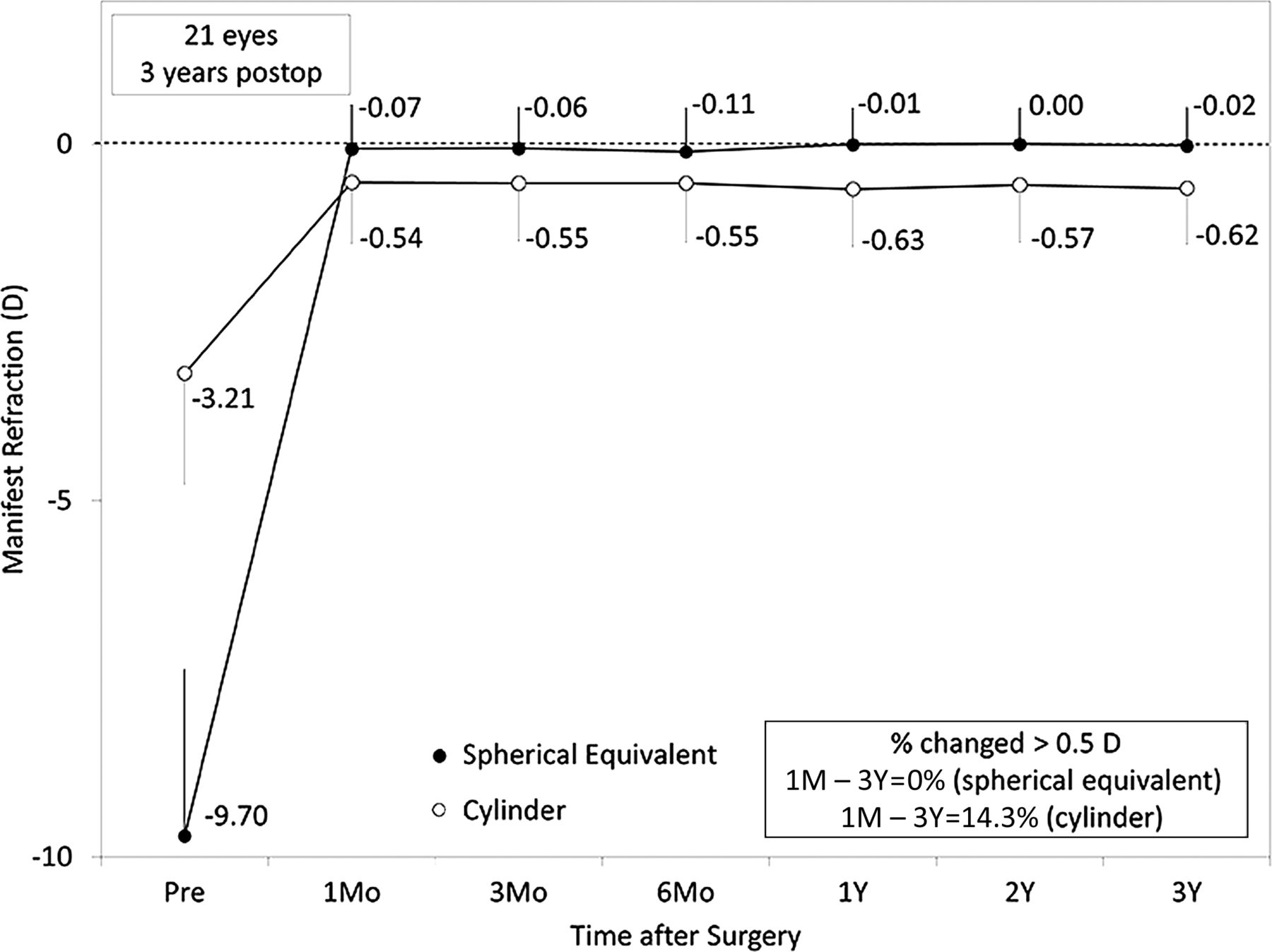
The change in the manifest spherical equivalent is shown in figure 5. At 1, 3 and 6 months and 1, 2 and 3 years postoperatively, the mean manifest spherical equivalent was −0.07±0.61, −0.06±0.57, −0.11±0.61, −0.01±0.50, 0.00±0.50 and −0.02±0.53 D, respectively (ANOVA, p=0.989). Changes in manifest refraction from 1 month to 3 years postoperatively were 0.04±0.33 D.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time courses of manifest spherical equivalent and refractive cylinder after toric posterior chamber phakic intraocular lens implantation in eyes with keratoconus. Mo, month; Y, year.
Astigmatism
The change in the manifest refractive cylinder is shown in figure 5. At 1, 3 and 6 months and 1, 2 and 3 years postoperatively, the mean manifest refractive cylinder was −0.54±0.86, −0.55±0.81, −0.55±0.83, −0.63±0.81, −0.57±0.80 and −0.62±0.79 D, respectively (ANOVA, p=0.998). Changes in manifest cylinder from 1 month to 3 years postoperatively were −0.08±0.41 D.
Surgically induced astigmatism
The amount of surgically induced astigmatism was 0.56±0.34 D (0.08–1.27 D) at an axis of 116.6°.
Intraocular pressure
The IOP was 10.9±2.3, 10.5±1.9, 11.4±2.2, 11.7±1.7, 12.1±2.2 and 11.1±1.9 mm Hg at 1, 3 and 6 months and 1, 2 and 3 years postoperatively, respectively (ANOVA, p=0.341). No significant increase in IOP (>23 mm Hg) occurred in any case during the observation period.
Keratometry
The mean keratometric reading was 46.5±1.9, 46.5±1.8, 46.5±1.8, 46.2±1.9, 46.4±2.5 and 46.0±2.1 D at 1, 3 and 6 months and 1, 2 and 3 years postoperatively, respectively (ANOVA, p=0.951). Corneal astigmatism was 3.0±1.6, 3.0±1.6, 3.0±1.5, 2.5±0.8, 2.7±0.6 and 2.5±0.7 D at 1, 3 and 6 months and 1, 2 and 3 years postoperatively, respectively (ANOVA, p=0.813).
Endothelial cell density
The endothelial cell density non-significantly fell from 2793±455 cells/mm2 preoperatively to 2653±494 cells/mm2 3 years postoperatively (Wilcoxon signed-rank test, p=0.074). The mean percentage of endothelial cell loss was 4.4% at 3 years postoperatively.
Secondary surgery or adverse events
All surgeries were uneventful and no significant intraoperative complication was observed. Deteriorating UDVA, changing refraction or 10° or more of axis rotation occurred in one eye (5%) postoperatively, and required ICL repositioning. No cataract formation, pigment dispersion glaucoma, pupillary block, axis misalignment, axis rotation, or any other vision-threatening complications were seen at any time during the observation period in this series.
Discussion
This study demonstrated the benefits of toric ICL implantation as regards safety, efficacy, predictability and stability in correcting spherical and cylindrical errors in cases of mild keratoconus throughout a 3-year observation period. These findings indicate that toric ICL implantation is a viable long-term surgical option for the treatment of refractive errors in patients with non-progressive mild keratoconus. We previously reported the 6-month clinical outcomes in 27 eyes of 14 patients with keratoconus.7 Three of these 14 patients did not complete the 3-year follow-up, but the visual and refractive outcomes following toric ICL implantation were almost equivalent to those of the remaining 11 patients in the current study. The previous visual and refractive outcomes following phakic IOL implantation as a single procedure for keratoconus are summarised in table 2. An extensive literature search suggests that this is one of the longest observational studies assessing the clinical outcomes of toric ICL implantation for mild and stable keratoconus. Our results have also confirmed that the postoperative shape of the cornea in patients with keratoconus was stable 3 years after toric ICL implantation. We were the first to present two cases of successful toric ICL implantation to correct high myopic astigmatism due to keratoconus.4 Alfonso et al5 ,6 also investigated visual outcomes after non-toric and toric ICL implantation in eyes with keratoconus. We7 and Hashemian et al10 have both shown that this type of implantation showed good safety, efficacy, predictability and stability for the correction of high myopia throughout a 6-month follow-up period in cases of keratoconus. Alió et al18 demonstrated that the mean safety and efficacy indices were 1.21±0.28 and 0.88±0.28, respectively, in an ICL group. Our current results are comparable with all previous findings regarding toric ICL implantation for keratoconus, but slightly inferior to those for toric ICL implantation for moderate to high myopic astigmatism, possibly because it is difficult to determine precisely the manifest refraction and the keratometric readings, with the result that the accuracy of toric ICL power calculation is reduced.
Summary of visual and refractive outcomes of phakic intraocular lens implantation for keratoconus as a single procedure
Regarding other phakic IOLs, a study of six keratoconic eyes by Budo et al19 showed that the reduction in spherical error was higher (87.4%) than in astigmatic error (64.5%) after iris-fixated toric phakic IOL implantation, suggesting that spherical errors are highly predictable but astigmatic errors only moderately so. Leccisotti and Fields20 were the first to report the implantation of angle-supported phakic IOLs as an effective method for correcting myopia in patients with keratoconus. However, they also reported no significant improvement in astigmatism after a 5.5-mm sclerocorneal incision was made. Moshirfar et al21 demonstrated that there was no change in postoperative astigmatism of +2.00 and +4.25 D after iris-fixated spherical phakic IOL implantation through a 5.5–6.0 mm incision. Kato et al22 stated that, 1 year postoperatively, approximately 86% of patients said they were ‘satisfied’ or ‘very satisfied’ with iris-supported phakic IOL implantation. Sedaghat et al23 reported that the mean final spherical and cylindrical refractions after iris-supported phakic IOL implantation were −0.03±1.81 and 2.08±1.04 D, respectively. Toric iris-supported phakic IOLs have an advantage over toric posterior chamber phakic IOLs in that there is no risk of postoperative IOL rotation thanks to the enclavation system on the iris. However, repositioning a toric ICL is easy and safe if axis alignment after implantation is incorrect. Alió et al18 found no statistical differences in the safety and stability results achieved with two types of iris-supported and posterior chamber phakic IOLs.
This study aimed primarily to determine whether the disease progresses with time in the selected study population, because this can induce changes in spherical and cylindrical refraction and/or higher-order aberrations, with the result that visual performance deteriorates. At no time during the 3-year follow-up period were any significant changes in manifest refraction or keratometry observed. Our results also suggest that no progression of the disease took place even in the late-postoperative period, possibly because the patients were all at least 30 years of age, and their eyes had had stable refraction for at least 1 year postoperatively. The usual perception of this disease is that it tends to slowly progress in the early stages but to stabilise later. We recently showed that ICL implantation does not have a significant effect on the corneal biomechanical parameters of either keratoconic or normal eyes.24 Budo et al19 recommended against performing phakic IOL implantation in either recently diagnosed keratoconus or younger patients with progressive keratoconus. Sedaghat et al23 suggested that phakic IOL implantation could be especially beneficial in patients with keratoconus and good preoperative CDVA, a high spherical-to-cylindrical ratio, and a higher than normal axial length. We believe that our criteria for selecting patients for the correction of refractive errors for mild keratoconus are appropriate for this technique, and that for this reason no progression of the disease occurred during a 3-year observation period. In the current study, the preoperative spherical equivalent refraction in three eyes (14%) showing a difference of >1.0 D with spherical equivalent correction was −11.13±3.33 D, and the preoperative cylinder in five eyes (24%) showing a difference of >1.0 D with astigmatic correction was −3.95±1.91 D, suggesting that the conditions of these eyes corresponded to keratoconus with higher myopia and astigmatism. It should be noted that toric ICL implantation is not suitable for advanced keratoconus, which is often accompanied by many higher-order aberrations due to the irregularly shaped cornea, and also corneal opacification, because the procedure aims to correct myopic and astigmatic errors alone. Penetrating or lamellar keratoplasty is probably a preferable surgical option for treating advanced keratoconus.
The use of intrastromal corneal rings and corneal collagen cross-linking are other viable options for the treatment of keratoconus. However, far less reduction in myopia and astigmatism is possible with intrastromal corneal rings or collagen cross-linking than with toric ICLs.8–14 A combination of intrastromal corneal rings or corneal cross-linking with phakic IOL implantation in a two-step procedure might also be effective in treating progressive keratoconus.25 ,26
In conclusion, our long-term clinical results suggest that the toric ICL performed well in correcting high myopic astigmatism in patients with mild and stable keratoconus over the entire 3-year observation period, and that no progression of the disease occurred, even in the late-postoperative period. These findings suggest that toric ICL implantation is a viable surgical option for the correction of myopic astigmatism for mild, stable keratoconus in a clinical setting.
References
Footnotes
-
Contributors KK, KS, AI, HK, TK, TN: design and conduct of the study; KK, AI, HK, MK, NA, TK, TN: collection, management, analysis and interpretation of the data; KK: preparation of the manuscript, KS, MK, NA: critical revision of the manuscript; KK, KS, AI, HK, MK, NA, TK, TN: final approval of the manuscript.
-
Funding This work was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology of Japan (24592642).
-
Competing interests Dr Shimizu is a consultant to STAAR Surgical Company. The other authors have no financial or proprietary interest in any material or method mentioned.
-
Ethics approval The study was approved by the Institutional Review Board of Kitasato University School of Medicine.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance