Article Text

Abstract
Aim: Vascular risk factors, and particularly vasospasm, are thought to play a part in the pathogenesis of normal pressure glaucoma (NPG). This study aimed to determine whether the function of systemic resistance arteries was altered in patients with NPG.
Methods: Contractile and relaxant function was assessed in arteries dissected from gluteal fat biopsies (11 NPG, 12 control) using small vessel myography.
Results: Responses to K+ and noradrenaline were similar in patients and controls and were unaffected by endothelial removal. In contrast, responses to 5-hydroxytryptamine (5-HT; pD2; 7.29 (SD 0.16) v 6.66 (0.19); p=0.03) and endothelin-1 (ET-1; pD2, 9.12 (0.10) v 8.72 (0.13); p=0.03) were enhanced in arteries from patients with NPG. Removal of the endothelium enhanced responses to 5-HT (pD2, 6.66 (0.19) v 7.66 (0.08); p=0.003) and ET-1 (pD2, 8.72 (0.13) v 9.66 (0.39); p=0.02) in control arteries but not in those from patients. ET-1 mediated contraction in control and patient arteries was reduced in the presence of (10−5 M) nifedipine. Endothelium dependent and independent relaxation was not impaired in arteries from patients.
Conclusions: This study has identified dysfunction of the systemic vascular endothelial cell in patients with normal pressure glaucoma. The vascular endothelium modulates contractile responses to 5-HT and ET-1 in human subcutaneous resistance arteries but this effect is lost in patients with NPG, indicating a selective defect in agonist mediated release of endothelium derived vasodilators. Selective antagonists of 5-HT and ET-1 may, therefore, help to prevent vasospasm in patients with NPG.
- vascular endothelium
- human resistance arteries
- normal pressure glaucoma
Statistics from Altmetric.com
Although glaucoma is generally associated with raised intraocular pressure, nearly one third of all glaucoma cases have normal eye pressure—a condition known as normal pressure glaucoma (NPG). It has been proposed that vascular dysfunction contributes to the pathogenesis of glaucoma and, in particular, NPG as this condition is associated with the presence of widespread cerebrovascular and systemic cardiovascular disease.1–3
It is conceivable that NPG is associated with a generalised vascular defect which produces alterations in both the ocular and systemic circulations. Functional abnormalities, including reduced blood flow velocity and increased resistance in a number of ocular arteries, have been demonstrated within the ophthalmic circulation of patients with NPG.4–6 Furthermore, the presence of optic disc haemorrhages has also been reported in patients with this condition.7,8 Functional abnormalities in the systemic circulation of patients with NPG are indicated by the high prevalence of migraine and Raynaud's disease, which are indicative of increased vasospasm in these individuals.9 Impaired systemic vascular function has been demonstrated in patients with NPG in whom blood flow in the fingers is reduced10,11 (both under basal conditions and following cold provocation) and endothelium dependent vasodilatation in the forearm is impaired.12 The relatively small number of studies to have assessed vascular reactivity and blood flow in the systemic circulation of these patients, however, prevents identification of the mechanisms underlying these abnormalities.
The mechanisms of vascular dysfunction have been investigated in a number of conditions, including hypertension13 and diabetes,14 using subcutaneous arteries isolated from biopsies of gluteal fat. This approach has the advantage of studying vascular dysfunction directly in arteries from patients (rather than animal models) and uses resistance arteries which contribute significantly to maintenance of blood pressure.15 Furthermore, removal of the endothelium makes it possible to determine whether functional abnormalities are the result of alterations in the vascular endothelial and/or smooth muscle cells.16 The authors are unaware, however, of any study which has used this technique to investigate systemic vascular dysfunction in NPG. This study aimed, therefore, to determine the nature of functional abnormalities in systemic resistance arteries isolated from patients with newly diagnosed NPG.
METHODS
Subjects
Eleven patients with newly diagnosed NPG were recruited for the study together with 12 healthy control subjects matched for age, sex, mean arterial blood pressure, and body weight. Patients with glaucoma had an intraocular pressure of less than 22 mm Hg on diurnal phasing, optic disc cupping with a characteristic pattern of visual field loss, and no history of previous ocular disease. All patients with NPG were assessed using a Goldmann applanation tonometer and the 24-2 threshold program on a Humphrey perimeter (Humphrey Instruments, Allergan Humphrey, San Leandro, CA, USA). Controls were recruited from among friends and relatives of patients participating in the study and by advertisement within the Royal Infirmary of Edinburgh. All control subjects had a normal ocular examination, intraocular pressure within normal limits, and intact visual fields on automated analysis. The patient group were either untreated (n = 7) or were being treated (n = 4) with β blockers (0.5% betaxolol hydrochloride (Betoptic), Alcon (UK) Ltd, Herts, UK); either alone (n = 3) or in combination with a carbonic anhydrase inhibitor (2% dorzolamide hydrochloride (Trusopt), Merck Sharp & Dohme, Herts, UK; n = 1). The four patients treated with β blockers did not take their medication on the day of the biopsy. Neither group was receiving any other topical treatment or any systemic vasoactive drugs and all were non-smokers. Samples of venous blood were obtained from some subjects for measurement of plasma cholesterol. The study protocol was approved by Lothian research ethics committee and conformed to the tenets of the Declaration of Helsinki. All subjects gave written informed consent before enrolment in the study.
Preparation of arteries
A biopsy of skin and subcutaneous fat (2 cm long × 1 cm × 1 cm) was taken from the gluteal region following subcutaneous injection of local anaesthetic (Xylocaine; 2% lidocaine hydrochloride with adrenaline, Astra Pharmaceuticals, Kings Langley, UK). Arteries were dissected from the biopsy and mounted as ring preparations (approximately 2 mm in length) on two 40 μm intraluminal stainless steel wires in a small vessel myograph (JP Trading, Aarhus, Denmark) for measurement of isometric tension. The vessels were bathed in physiological salt solution (PSS; composition in mM: NaCl 119, KCl 4.7, MgSO4 1.17, KH2PO4 1.18, d-glucose 5.5, K2 EDTA 0.026, NaHCO3 25, CaCl2 2.5) maintained at 37°C and gassed with 95% oxygen, 5% carbon dioxide. The length of each vessel segment was measured by light microscopy using a travelling micrometre eyepiece. Following a 30 minute equilibration period, the resting tension-internal circumference relation was determined for each artery by stepwise stretching of the vessel and application of the LaPlace equation as previously described.17 From this, the internal circumference (L100) that the artery would have in situ when relaxed under a transmural pressure of 100 mm Hg (13.3 kPa) was calculated. Each vessel was then set to an internal circumference of 0.9L100 at which these vessels develop maximum active tension.18
The vessels were allowed to equilibrate at their optimum resting tension for 30 minutes before undergoing a standard start protocol in which the viability of each artery was assessed. This consisted of stimulating the vessels twice with NAK (a high potassium solution (125 mM; KPSS), prepared by equimolar substitution of KCl for NaCl in normal PSS, containing noradrenaline (NA; 5 × 10−6 M)), once with NA (5 × 10−6 M) alone, once with KPSS alone, and a final time with NAK. The vessels were washed and allowed to relax fully between each activation. In some arteries the endothelium was removed by gently rubbing the lumen of the vessel with a human hair. Histological studies have confirmed that this method successfully removes the endothelium16 and denudation was confirmed in the present study by the failure of the vessel to relax in response to acetylcholine (ACh) or bradykinin (BK).
Experimental protocol
Cumulative concentration-response curves were obtained to the constrictor agonists 5-hydroxytryptamine (5-HT; 10−9–3 × 10−5 M), NA (10−9–3 × 10−5 M, endothelin-1 (ET-1; 10−11–3 × 10−7 M), and K+ (10–125 mM) in both endothelium intact and denuded vessels. In endothelium intact arteries concentration-response curves to ET-1 were obtained either in the absence of or following 10 minutes' incubation with the calcium channel blocker nifedipine (10−5 M). Cumulative concentration-response curves were also obtained for the endothelium dependent dilators ACh (10−9–3 × 10−5 M) and BK (10−10–3 × 10−6 M) and for the endothelium independent nitric oxide donor 3-morpholinosydnonimine (SIN-1; 10−8–10−4 M) following contraction of the arteries with a submaximal concentration of NA (10−7–10−6 M). Following each concentration-response curve the vessels were washed thoroughly with PSS and allowed to relax fully for at least 20 minutes before the next drug was tested.
Drugs
All salts were obtained from BDH (Poole, Dorset, UK). Noradrenaline bitartrate, 5-hydroxytryptamine creatinine sulphate complex, acetylcholine chloride, bradykinin acetate, and nifedipine were from Sigma (Poole, Dorset, UK). Endothelin-1 and 3-morpholinosydnonimine hydrochloride were obtained from Alexis Biochemicals (Beeston, Nottingham, UK). All drugs were dissolved in deionised water except for ET-1 which was dissolved in 50% methanol and nifedipine which was dissolved in 50% ethanol before subsequent dilution in deionised water. Final bath concentrations of methanol and ethanol did not exceed 1.5% and 0.5% v/v, respectively.
Statistical analysis
Contractile responses are expressed as active force (mN/mm) and as a percentage of the maximum response to NAK obtained during the standard start (% max NAK). Relaxations are expressed as a percentage of the induced precontraction to NA. For each concentration-response curve the molar concentration required to produce 50% of the maximum contraction (EC50) or relaxation (IC50) was calculated by fitting the Hill equation using the curve fitting program Fig P (Biosoft, UK). The sensitivity of the vessels to each agonist was expressed as the negative logarithm of the EC50 (pD2) for constrictor agonists or −log IC50 for dilator agonists. All results are given as the mean (SEM) for n experiments, where n represents the number of subjects. Maximum responses and EC50 values were compared using Student's unpaired t test and differences considered significant when p≤0.05.
RESULTS
There were no significant differences in the demographics between patient and control groups (Table 1). The internal diameters of resistance arteries isolated from gluteal biopsies used in this study were similar (p=0.53) in patients with glaucoma (258 (SEM 17) μm) and control subjects (238 (26) μm), and the contractile responses evoked by NAK were not significantly different between the two groups (patients 3.06 (0.22) mN/mm; controls 2.66 (0.29) mN/mm, p=0.26).
Characteristics of control subjects and patients with NPG
Responses to dilator agonists
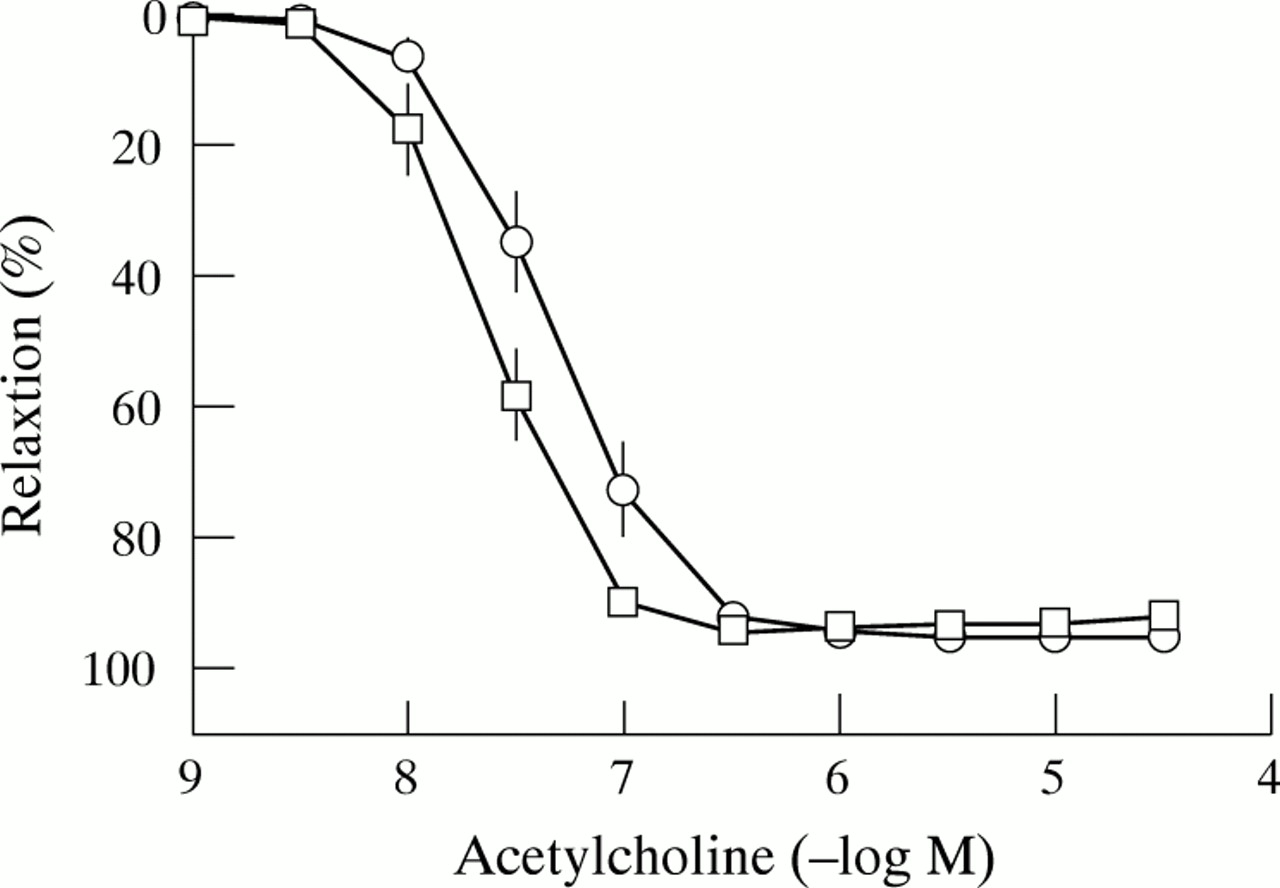
ACh, BK, and SIN-1 all evoked concentration dependent relaxations in arteries precontracted with NA from both patients and controls. The relaxation in response to ACh and BK was significantly reduced following removal of the endothelium in both subject groups whereas the response to SIN-1 was unaffected (Table 2). Arteries from patients with glaucoma were significantly more sensitive (p=0.03) to ACh than controls; the maximum relaxation, however, was similar in the two groups of subjects (Table 2; Fig 1). Neither maximum relaxation nor sensitivity to either the endothelium dependent dilator, BK, or to the endothelium-independent dilator, SIN-1, were significantly different in arteries from patients compared with those from controls (Table 2).
Maximum relaxation and sensitivity (−log IC50) values for dilator agonists in endothelium intact and denuded arteries isolated from control subjects and patients with NPG

Cumulative concentration-response curves to acetylcholine in endothelium intact arteries isolated from control subjects (ˆ; n = 11) and patients with NPG (□; n = 11). Each point represents the mean with SEM shown by vertical bars.
Responses to constrictor agonists
All arteries produced concentration dependent contractions in response to NA, 5-HT, ET-1, and K+. The maximum responses and sensitivities to NA and K+ did not differ between arteries from control subjects and patients with glaucoma (Table 3). In addition, removal of the endothelium had no effect on maximum contractile response or sensitivity to these agonists in either control or patient groups (Table 3).
Maximum contractile responses (Emax) and sensitivity (pD2) values for constrictor agonists in endothelium intact and denuded arteries isolated from control subjects and patients with NPG
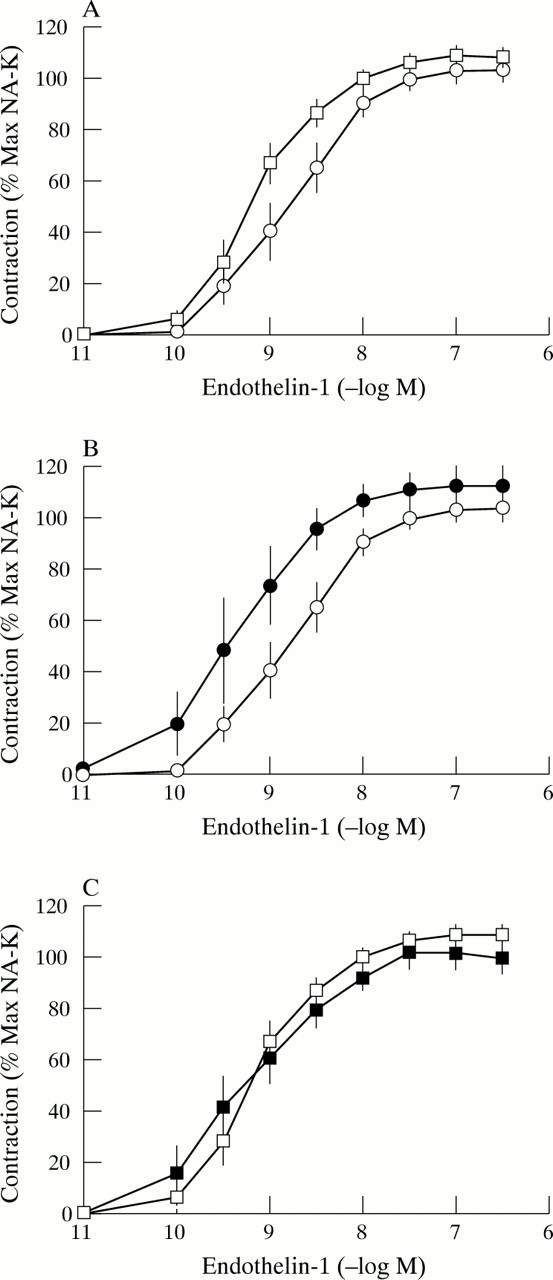
Arteries from patients with glaucoma were more sensitive to 5-HT (p = 0.03) and the maximum contractile response to this agonist was greater (p = 0.03) when compared with arteries from control subjects (Table 3; Fig 2A). Removal of the endothelium from control vessels caused a significant increase in maximum contractile response (p = 0.045) and sensitivity (p = 0.003) to 5-HT (Table 3; Fig 2B) whereas endothelial removal from vessels from patients had no effect on either maximum response (p=0.66) or sensitivity (p=0.22; Table 3; Fig 2C).

Cumulative concentration-response curves to 5-HT in (A) endothelium intact arteries isolated from control subjects (ˆ; n = 8) and patients with NPG (□; n = 8), (B) endothelium intact (ˆ; n = 8) and denuded arteries (•; n = 5) isolated from control subjects and (C) endothelium intact (□; n = 8) and denuded arteries (▪; n = 6) isolated from patients with NPG. Each point represents the mean with SEM shown by vertical bars.
ET-1 evoked contractions were of similar magnitude (p=0.61) in arteries from patients with glaucoma and control subjects; the arteries from patients were, however, significantly more sensitive (p = 0.03) to ET-1 than control arteries (Table 3; Fig 3A). Comparison of individual concentration-response curves indicated that responses to ET-1 were similar in arteries from patients previously receiving betaxolol HCl and those from untreated patients. Endothelial removal from control vessels caused a 10-fold increase in sensitivity (p=0.02) to ET-1 (Table 3; Fig 3B); denudation of vessels from patients, however, had no effect on sensitivity (p = 0.43) to this agonist (Table 3; Fig 3C). In endothelium intact arteries the maximum contraction in response to ET-1 was reduced following incubation with nifedipine (10−5 M) in both patients (Emax reduced from 3.45 (0.39) to 1.79 (0.32) mN/mm; n = 7; p=0.008) and controls (Emax reduced from 3.13 (0.49) to 1.65 (0.31) mN/mm; n = 6; p=0.04).
{kind=link}
{kind=link}
{kind=link}
Cumulative concentration-response curves to ET-1 in (A) endothelium intact arteries isolated from control subjects (ˆ; n=9) and patients with NPG (□; n=10), (B) endothelium intact (ˆ; n=9) and denuded arteries (•; n=5) isolated from control subjects and (C) endothelium intact (□; n=10) and denuded arteries (▪; n=6) isolated from patients with NPG. Each point represents the mean with SEM shown by vertical bars.
DISCUSSION
A number of studies have suggested that alterations in the systemic vasculature contribute to the aetiology and progression of NPG. Indeed, treatment with drugs that increase systemic blood flow can also improve visual field in some patients with NPG.19 This investigation, the first to describe vascular function in arteries isolated from patients with NPG, aimed to determine whether the functional characteristics of isolated resistance arteries were altered in patients with this condition.
The demonstration that endothelium dependent relaxation was maintained (indeed sensitivity to ACh was enhanced) indicates that the ability of the endothelium to release relaxing factors is not impaired in arteries from patients with NPG. The cause of the selective increase in sensitivity to ACh remains unclear but may reflect an alteration at the level of the muscarinic receptor itself or in muscarinic receptor mediated release of endothelium derived relaxing factors. Certainly, the ability of the smooth muscle to relax in response to nitric oxide (NO) is not altered as responses to the NO donor, SIN-1, were unchanged in arteries from patients with NPG. These results contrast with a study of forearm blood flow in vivo performed by our own group12 which reported impaired ACh mediated relaxation (due to an abnormality in endothelial cell function) in patients with NPG.12 This is particularly relevant as some of the patients in whom forearm blood flow was assessed also provided biopsies for the present investigation. The reasons for the differences between the in vivo study and the present in vitro investigation are unclear but reflect similar disparities reported between in vitro and in vivo studies of vascular function in hypertension,13,20 insulin dependent diabetes mellitus (IDDM),21,22 and non-insulin dependent diabetes mellitus (NIDDM).14,23 As small vessel myography isolates resistance arteries from the humoral environment, it is possible that impaired ACh mediated relaxation in vivo is caused by enhanced degradation of endothelium derived NO by bloodborne factors (for example, free radicals). Alternatively, functional responses obtained using arteries suspended on intraluminal wires in vitro may not reflect the behaviour of those in vivo. However, even when pressure myography (which places the isolated arteries under conditions similar to those experienced in vivo) was used to assess vascular function in patients with NIDDM,14 the results did not correspond with those obtained using forearm plethysmography.23 Finally, disparities between studies using forearm blood flow and isolated resistance arteries may reflect physiological variations between vessels of differing anatomical origin. Blood flow in the forearm occurs mainly through muscular arteries (with only a small contribution through cutaneous or subcutaneous vessels),24 whereas gluteal biopsies provide purely subcutaneous arteries. In the latter, ACh stimulates relaxation mainly via the action of endothelium derived hyperpolarising factor (EDHF) with a relatively small component mediated by NO.25 ACh also acts via endothelium derived NO in the forearm but the contribution of EDHF has not been determined in this territory.26 While the relative contributions of NO and EDHF to relaxation of arteries from control subjects and patients with NPG require further investigation, it is possible that impaired NO mediated relaxation in NPG (demonstrated in the forearm12) is masked in gluteal subcutaneous resistance arteries by enhanced EDHF activity.
The endothelium plays an important part in the control of local vascular tone and blood flow27 and many vasoconstrictors modulate their own action by receptor mediated release of endothelium derived relaxing factors. Removal of the endothelium attenuates this modulatory effect, resulting in augmented agonist mediated contraction.28 The present study used a receptor independent vasoconstrictor, K+, which is unaffected by either basal or stimulated release of NO, as well as 5-HT, ET-1, and NA, which cause contraction by stimulating receptors (5-HT2A, ETA and ETB, and α1 adrenoceptors, respectively) on the vascular smooth muscle. In some arteries, contractile responses to 5-HT, ET-1, and NA are modulated by (5-HT2C,29 ETB,30 and α1 and α2 adrenoceptor31) receptor mediated release of NO and PGI2 from the endothelium. Adrenoceptor mediated release of endothelium derived relaxing factors was not significant in the present study as responses to NA were unaffected by removal of the endothelium. This contrasts with reports of enhanced sensitivity to NA in denuded human subcutaneous resistance arteries14 mounted in a pressure myograph (probably because of a greater effect of basal NO release than in the wire system used in the present study). The enhanced contractile responses to 5-HT and ET-1 following endothelial cell removal indicated that, in human gluteal subcutaneous resistance arteries, the vascular endothelium modulates contraction to these agonists. The loss of this modulatory effect in arteries from patients with NPG indicates an impairment in receptor mediated release of endothelium derived relaxing factors.
The selective enhancement of contractile responses (to 5-HT and ET-1 but not to NA or K) in arteries from patients with NPG is strikingly similar to results obtained in resistance arteries from patients with hypertension.13 Furthermore, Angus et al13 also reported normal endothelium dependent relaxation in arteries from hypertensive individuals. The unaltered contraction with K+ and NA indicates that smooth muscle responsiveness was not enhanced in patients with NPG, an observation confirmed by the similar contractile responses to NA, 5-HT, and ET-1 in denuded arteries. The altered contractile responses observed in patients with NPG were only found with agonists which, in control arteries, were shown to exhibit enhanced contraction following endothelial cell removal. Therefore, the enhanced responses to 5-HT and ET-1 observed in intact arteries from patients with NPG must be due to alterations at the level of the endothelial cell. An increase in the release of endothelium derived constrictor prostanoids cannot account for the enhanced responsiveness to 5-HT and ET-1 in arteries from patients with NPG, since removal of the endothelium did not reduce these responses. Since only the responses to 5-HT and ET-1, but not that to NA, were augmented, the impairment is probably due to alterations in endothelial 5-HT2C and ETB receptor function or in intracellular signal transduction mechanisms rather than to a non-specific reduction in the release of dilating substances. This is supported by the observation that endothelium dependent relaxations to ACh and BK were not impaired in arteries from patients with NPG. These findings may also have relevance for the ocular and extraocular circulations as 5-HT mediated contraction is modulated by endothelial nitric oxide synthase in the porcine ophthalmic arteries32 and low doses of ET-1 cause dilatation (probably by ETB receptor mediated NO release from the endothelium) in the perfused porcine eye.33
The increased sensitivity to ET-1 observed in the present study, together with the increased circulating levels of ET-134 and the abnormal response to postural change35 reported in patients with NPG, could result in enhanced vasoconstriction and contribute to the vasospasm seen in some patients with this condition. Interventions which reduce the effects of this peptide may, therefore, be useful in the treatment of such patients. The contractile response to ET-1 was only partially blocked by the calcium antagonist, nifedipine. This indicates that ET-1 induced contraction in this artery is mediated in part by an influx of extracellular calcium through voltage operated calcium channels but mainly through other mechanisms, such as the activation of phospholipase C and the release of intracellular calcium. Calcium channel blockers may, therefore, be of limited benefit in reducing ET-1 induced vasospasm. This may suggest a role for selective ET receptor antagonists in the treatment of patients with NPG.
In conclusion, this investigation demonstrated that endothelium dependent modulation of receptor mediated contraction is selectively reduced in subcutaneous resistance arteries isolated from patients with NPG. This occurs despite unaltered endothelium dependent relaxation and suggests alterations in receptor populations on the vascular endothelium. This study complements the investigation of forearm blood flow in patients with NPG,12 as both demonstrate impaired systemic vascular function. While neither study confirmed that the systemic vascular defects identified are responsible for optic nerve damage both support the hypothesis that NPG is one manifestation of more widespread vascular abnormalities. Enhanced contractile responses in the periphery may contribute to vascular complications in these patients and further studies are required to assess whether 5-HT and ET-1 receptor antagonists may be useful in the prevention of vasospasm.
Acknowledgments
Supported by the Royal National Institute for the Blind (London, UK).
REFERENCES
Linked Articles
- BJO at a glance