
Abstract
Objective
We estimated the quality of life impact of vision loss in a community-based population with diabetes.
Design and methods
We randomly surveyed 4,000 members of a large health maintenance organization with type 2 diabetes to assess quality of life using the EQ-5D instrument. Visual acuity was obtained by automated text processing of clinical notes recorded during the two years preceding subjects’ surveys. Natural language processing was used to collect data from electronic medical records and to read clinical notes to determine the stage of retinopathy. Linear regression was used to model quality of life scores.
Results
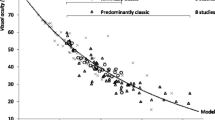
Of the 4,000 surveys sent, approximately 55% of patients responded. Patients with ≥20/20 acuity reported the highest mean utility (mean = 0.82), which declined as the visual angle doubled to 20/40 (mean = 0.75), and then doubled again to ≤20/80 (mean = 0.71). Perfect utility (1.0) was reported by 28% of the sample. Only 7% of patients suffered visual impairment (≤20/40), and lower levels of visual acuity rarely occurred. Compared with patients with ≥20/20 acuity, the first doubling of the visual angle (20/40) lowered utility by three points (95% confidence interval [CI], −0.05 to −0.01), and the second doubling of the visual angle (≤20/80) lowered utility by six points (95%CI, −0.10 to −0.02).
Conclusions
This study aimed to estimate disutility associated with visual loss in patients with diabetes using a community-based sample and controlled for many characteristics associated with quality of life. We found a smaller utility decrement compared to other studies, suggesting that visual acuity’s impact on the quality of life for patients with diabetes in the community setting differs from more selected populations.


Similar content being viewed by others


References
Congdon, N. G., Friedman, D. S., & Lietman, T. (2003). Important causes of visual impairment in the world today. Journal of the American Medical Association, 290(15), 2057–2060. doi:10.1001/jama.290.15.2057.
Congdon, N., O’Colmain, B., Klaver, C. C., et al. (2004). Causes and prevalence of visual impairment among adults in the United States. Archives of Ophthalmology, 122(4), 477–485. doi:10.1001/archopht.122.4.477.
Klein, R., Klein, B. E., Moss, S. E., et al. (1984). The Wisconsin epidemiologic study of diabetic retinopathy. III. Prevalence and risk of diabetic retinopathy when age at diagnosis is 30 or more years. Archives of Ophthalmology, 102(4), 527–532.
Coyne, K. S., Margolis, M. K., Kennedy-Martin, T., et al. (2004). The impact of diabetic retinopathy: perspectives from patient focus groups. Family Practice, 21(4), 447–453. doi:10.1093/fampra/cmh417.
Brown, G. C., Sharma, S., Brown, M. M., et al. (2000). Utility values and age-related macular degeneration. Archives of Ophthalmology, 118, 47–51.
Sharma, S., Oliver-Fernandez, A., Bakal, J., et al. (2003). Utilities associated with diabetic retinopathy: results from a Canadian sample. The British Journal of Ophthalmology, 87(3), 259–261. doi:10.1136/bjo.87.3.259.
Sharma, S., Brown, G. C., Brown, M. M., et al. (2000). Converting visual acuity to utilities. Canadian Journal of Ophthalmology, 35(5), 267–272.
U.K. Prospective Diabetes Study Group (1999). Quality of life in type 2 diabetic patients is affected by complications but not by intensive policies to improve blood glucose or blood pressure control (UKPDS 37). Diabetes Care, 22(7), 1125–1136. doi:10.2337/diacare.22.7.1125.
Clarke, P. M., Simon, J., Cull, C. A., et al. (2006). Assessing the impact of visual acuity on quality of life in individuals with type 2 diabetes using the short form-36. Diabetes Care, 29(7), 1506–1511. doi:10.2337/dc05-2150.
Bagust, A., & Beale, S. (2005). Modelling EuroQol health-related utility values for diabetic complications from CODE-2 data. Health Economics, 14(3), 217–230. doi:10.1002/hec.910.
Clarke, P., Gray, A., & Holman, R. (2002). Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Medical Decision Making, 22(4), 340–349. doi:10.1177/027298902400448902.
Coffey, J. T., Brandle, M., Zhou, H., et al. (2002). Valuing health-related quality of life in diabetes. Diabetes Care, 25(12), 2238–2243. doi:10.2337/diacare.25.12.2238.
Greenlick, M., Freeborn, D., & Pope, C. (1998). Health care research in an HMO: Two decades of discovery. Baltimore: Johns Hopkins University Press.
Brown, J. B., Nichols, G. A., & Glauber, H. S. (2000). Case-control study of 10 years of comprehensive diabetes care. The Western Journal of Medicine, 172(2), 85–90. doi:10.1136/ewjm.172.2.85.
Brooks, R. (1996). EuroQol: the current state of play. Health Policy (Amsterdam), 37(1), 53–72. doi:10.1016/0168-8510(96)00822-6.
Shaw, J. W., Johnson, J. A., & Coons, S. J. (2005). US valuation of the EQ-5D health states: development and testing of the D1 valuation model. Medical Care, 43(3), 203–220. doi:10.1097/00005650-200503000-00003.
Bastyr, E. J., III, Stuart, C. A., Brodows, R. G., et al. (2000). Therapy focused on lowering postprandial glucose, not fasting glucose, may be superior for lowering HbA1c. IOEZ Study Group. Diabetes Care, 23(9), 1236–1241. doi:10.2337/diacare.23.9.1236.
Hazlehurst, B., Frost, H. R., Sittig, D. F., et al. (2005). MediClass: a system for detecting and classifying encounter-based clinical events in any electronic medical record. Journal of the American Medical Informatics Association, 12(5), 517–529. doi:10.1197/jamia.M1771.
Wilkinson, C. P., Ferris, F. L., III, Klein, R. E., et al. (2003). Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology, 110(9), 1677–1682. doi:10.1016/S0161-6420(03)00475-5.
Rothman, K. J., & Greenland, S. (1998). Modern epidemiology (2nd ed.). Boston: Lippincott Williams & Wilkins.
Brazier, J., Roberts, J., & Deverill, M. (2002). The estimation of a preference-based measure of health from the SF-36. Journal of Health Economics, 21(2), 271–292. doi:10.1016/S0167-6296(01)00130-8.
Acknowledgments
We thank Ms. Kim Olson of the Center for Health Research for performing the chart abstractions. We are grateful to Dr. William Borok of Kaiser Permanente Northwest for his clinical advice. Drs. Matthew Rousculp and Honjun Kan—who were employed by Eli Lilly and Company at the time of the study—provided helpful comments on earlier versions of the manuscript.
While this research does not contain evaluations of any products, Eli Lilly and Company supported the research through a contract to the Center for Health Research, Kaiser Permanente Northwest. The contract between Eli Lilly and Company and the Center for Health Research protected the Center for Health Research’s right to publish the findings.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Smith, D.H., Johnson, E.S., Russell, A. et al. Lower visual acuity predicts worse utility values among patients with type 2 diabetes. Qual Life Res 17, 1277–1284 (2008). https://doi.org/10.1007/s11136-008-9399-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-008-9399-1