- 1 Manchester Royal Eye Hospital, Manchester University NHS Foundation Trust, Manchester, UK
- 2 School of Healthcare Sciences, Cardiff University, Cardiff, UK
- 3 Bristol Eye Hospital, University Hospitals Bristol NHS Foundation Trust, Bristol, UK
- Correspondence to Patrick J G Gunn; patrick.gunn{at}cmft.nhs.uk
- Received 2 October 2017
- Revised 18 December 2017
- Accepted 3 January 2018
Abstract
Objective The purpose of this paper is to describe the findings of a national survey that aimed to estimate the proportion of Hospital Eye Service (HES) units using glaucoma virtual clinics, to determine how these services differ and to gauge clinicians’ views and opinions on the safety and acceptability of this model of care compared with usual care.
Methods and analysis This 12-question survey was disseminated nationally to 92 clinical lead consultant ophthalmologists using SurveyMonkey.
Results The response rate was 45.7%. There were 21 out of the total 42 respondents (50.0%) who were based at an NHS Trust where glaucoma virtual clinics were already being used and a further 9 (21.4%) were planning to establish one. Clinical leads largely rated efficiency and patient safety to be at least equivalent to usual care (92.9%) and 81.0% perceived glaucoma virtual clinics to be acceptable to patients. The main reasons for not running glaucoma virtual clinics were insufficient staff (71.4%) and inadequate space (47.6%). The majority of those running virtual clinics used this model of care for ‘lower risk’ patients such as ocular hypertensives (90.5%) and glaucoma suspects.
Conclusion Glaucoma virtual clinics are employed by a large proportion of HES units, with many seeking to develop such services. Clinical leads largely rate efficiency, patient safety and the perception of patient acceptability to be at least equivalent to usual care.
- glaucoma
- telemedicine
Key messages
What is known already about this subject?
To date, there has been little evidence about how widespread the use of the virtual clinic model has become in caring for patients with glaucoma.
What are the new findings?
This study has shown glaucoma virtual clinics are currently employed by a large proportion of Hospital Eye Service units, with many other units seeking to develop such services.
Clinical leads largely rate efficiency, patient safety and the perception of patient acceptability to be at least equivalent to usual care in glaucoma.
The Standards Panel’s recommendations for glaucoma virtual clinics appear to be being adopted by most units running glaucoma virtual clinics.
How might these results change the focus of research or clinical practice?
Given the rapid expansion of virtual clinics in caring for people with glaucoma, qualitative studies are necessary to better understand how patients at different disease stages, as well as clinicians, experience and perceive virtual glaucoma clinics, thus further informing approaches to this model of care.
Background
Providing sufficient appointment capacity for the management of glaucoma is a considerable challenge for providers of ophthalmic healthcare. In England alone, there are an estimated 480 000 cases of chronic open angle glaucoma and 0.75 to 1.2 million cases of ocular hypertension and glaucoma suspects (GSs), all of whom require some form of service to manage either their actual disease or their risk of disease.1 In 2009, a National Patient Safety Agency rapid response report2 raised concerns about delays to follow-up for patients with glaucoma and the risk of sight loss and both an Royal National Institue of Blind People (RNIB) survey3 and a Royal College of Ophthalmologists clinical leads survey4 also identified significant concerns about delivering appropriate capacity for glaucoma review visits.
It is widely recognised that caring for people with glaucoma is an enormous task that requires multiprofessional collaboration as well as innovations in service delivery. One such innovation is the ‘virtual’ clinic which, in the case of glaucoma, usually takes the form of patient follow-up attendances either in a hospital clinic or in a community clinic, including services that make use of a mobile clinic facility. In these models of care, some of which use electronic patient records (including web-based data recording), patient data are collected by technicians, ophthalmic nurses and/or non-specialist orthoptists or optometrists, with subsequent consultant ophthalmologist/expert clinician data review and decision-making.5 These clinics are intended to maximise appointment capacity and reduce waiting times, provide a ‘one stop shop’ with all tests being performed in one session and help to optimise the discharge rate by using consultant review. The virtual model has also been used to refine6 and triage7 community referrals. There is, however, a paucity of information on the number of clinics that have been established in the UK and how safe and acceptable such services are considered to be. The purpose of this paper is to describe the findings of a national survey of clinical leads that aimed to estimate the proportion of Hospital Eye Service (HES) units using, or considering the use of, glaucoma virtual clinics, to determine how these services differ and to gauge lead clinicians’ views and opinions on the safety and acceptability of this model of care compared with usual care.
Methods
A survey comprising 11 questions was developed by a team of glaucoma specialist clinicians. This survey sought information about acceptability and use of new models of care before seeking more detail on current use of virtual glaucoma clinics and the scope of practice therein. Clinicians were given a choice of fixed response categories to select from as well as the option to provide additional information or comments in free text. A summary of the questions asked is detailed in figure 1.

Summary of questions asked in clinical/glaucoma leads’ survey. Clinical leads were asked to respond to this series of questions using the SurveyMonkey online platform. NHS, National Health Service; PDS, pigment dispersion syndrome; PXF, pseudoexfoliation.
This survey was disseminated nationally to 92 clinical lead consultant ophthalmologists using the SurveyMonkey online survey platform. Clinical leads were offered the opportunity to delegate responsibility for completing the survey to the glaucoma lead if deemed more appropriate. The survey was distributed in February 2016 with two subsequent reminder emails at 2 and 6 weeks after the initial invitation and with the survey remaining open until 17 April 2016. The survey did not include private providers contracted to provide National Health Service (NHS) care, only NHS Trusts. The survey was reviewed and approved by the Royal College of Ophthalmologists in accordance with their policy on surveying members.
Results
Glaucoma virtual clinic implementation and location
There were 42 respondents from clinical/glaucoma leads, representing an overall response rate of 45.7%. A total of 21 respondents (50.0%) were primarily based at an acute trust/major teaching hospital and 50.0% were based at district general hospitals. Twenty one (50.0%) respondents were based at an NHS Trust where glaucoma virtual clinics were already being used, 17 of which (81.0%) were based at acute trust/major teaching hospitals. Only 4 respondents out of 21 (19.0%) working at a district general hospital were operating a glaucoma virtual clinic. Of those HES units not currently operating a glaucoma virtual clinic, 9 out of 21 respondents (42.9%) were planning to establish one. There was a spread of how well established the glaucoma virtual clinics were, with 5 out of 21 respondents (23.8%) having established their virtual clinic more than 5 years ago. There appears to have been a large increase in virtual clinic implementation in the last few years, with 13 out of 21 respondents (61.9%) having established clinics within the past 3 years. A total of 6 out of 21 respondents (28.6%) ran their virtual service from community clinics and 2 out of 21 respondents (9.5%) from a mobile unit. No respondents reported using a community optometry practice.
Glaucoma virtual clinic efficiency, safety and patient acceptability
Out of 42 respondents, 39 (92.9%) rated the efficiency of glaucoma virtual clinics to be at least similar to that of standard care, with some 31.0% (13/42 respondents) rating their efficiency as very good. In terms of patient safety, 39 out of 42 respondents (92.9%) rated glaucoma virtual clinics to be at least similar to standard care. Only 3 out of 42 respondents (7.1%) described both their efficiency and safety as poor.
Clinicians were also asked to consider their perception of patients’ acceptability of glaucoma virtual clinics. Of the 42 respondents, 34 (81.0%) considered patients’ acceptability of such clinics to be at least similar to that of usual care, although 8 (19.0% respondents) rated this acceptability to be poor (figure 2).
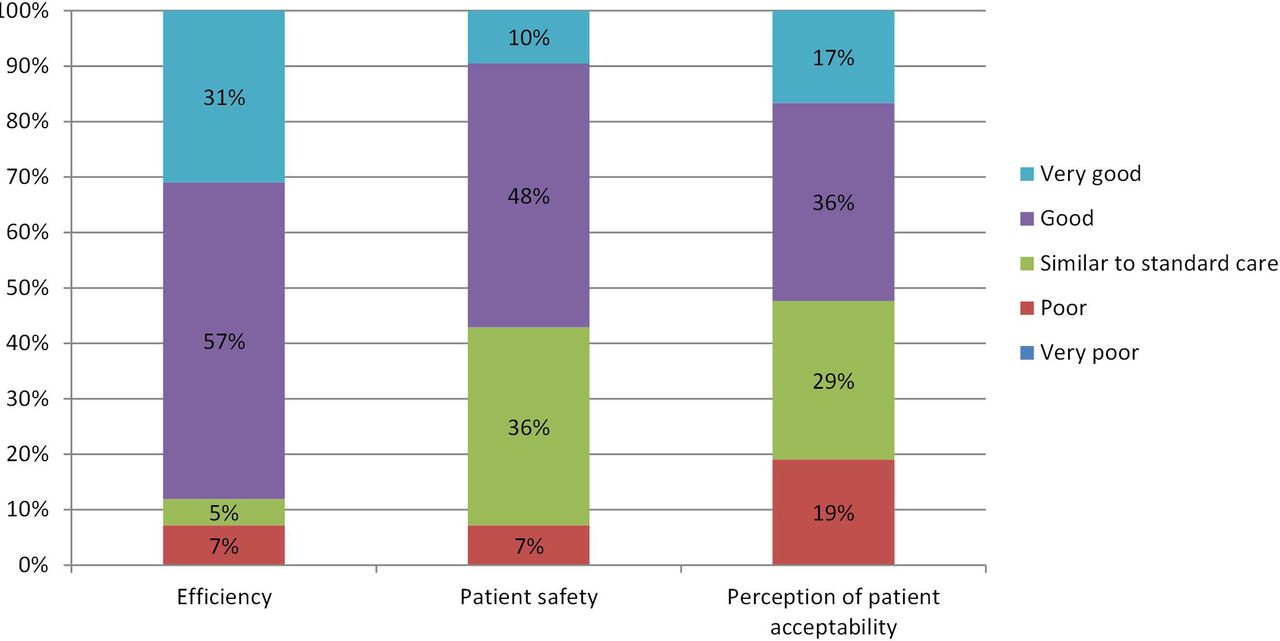
How would you rate glaucoma virtual clinics (n=42)? Respondents were asked how they rated glaucoma virtual clinics in terms of efficiency, patient safety and perception of patient acceptability on a five-point Likert scale from very bad to very good.
Reasons for not running glaucoma virtual clinics
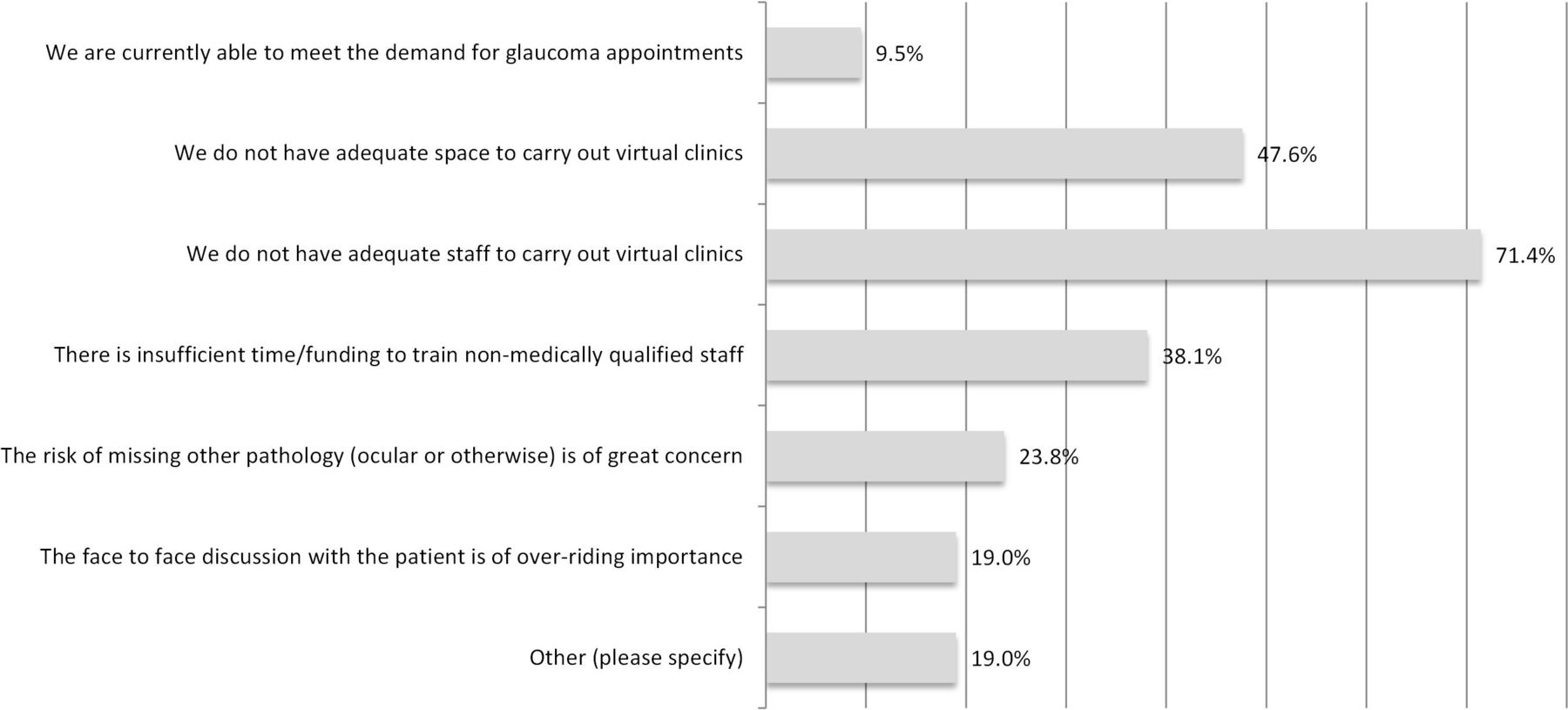
There were 21 respondents from ophthalmology units of NHS Trusts who were not running glaucoma virtual clinics. The main reasons reported for lack of adoption were insufficient staff (15 out of 21 respondents; 71.4%), inadequate space (10 out of 21 respondents; 47.6%) and insufficient time/funding to train non-medically qualified staff (8 out of 21 respondents; 38.1%). The risk of missing pathology (ocular or other) was of great concern to 5 out of 21 respondents (23.8%) and 4 out of 21 respondents (19.0%) considered the face-to-face discussion with patients to be of over-riding importance. Only 2 out of 21 respondents (9.5%) reported having adequate capacity to meet the demand for appointments. This data are summarised in figure 3.
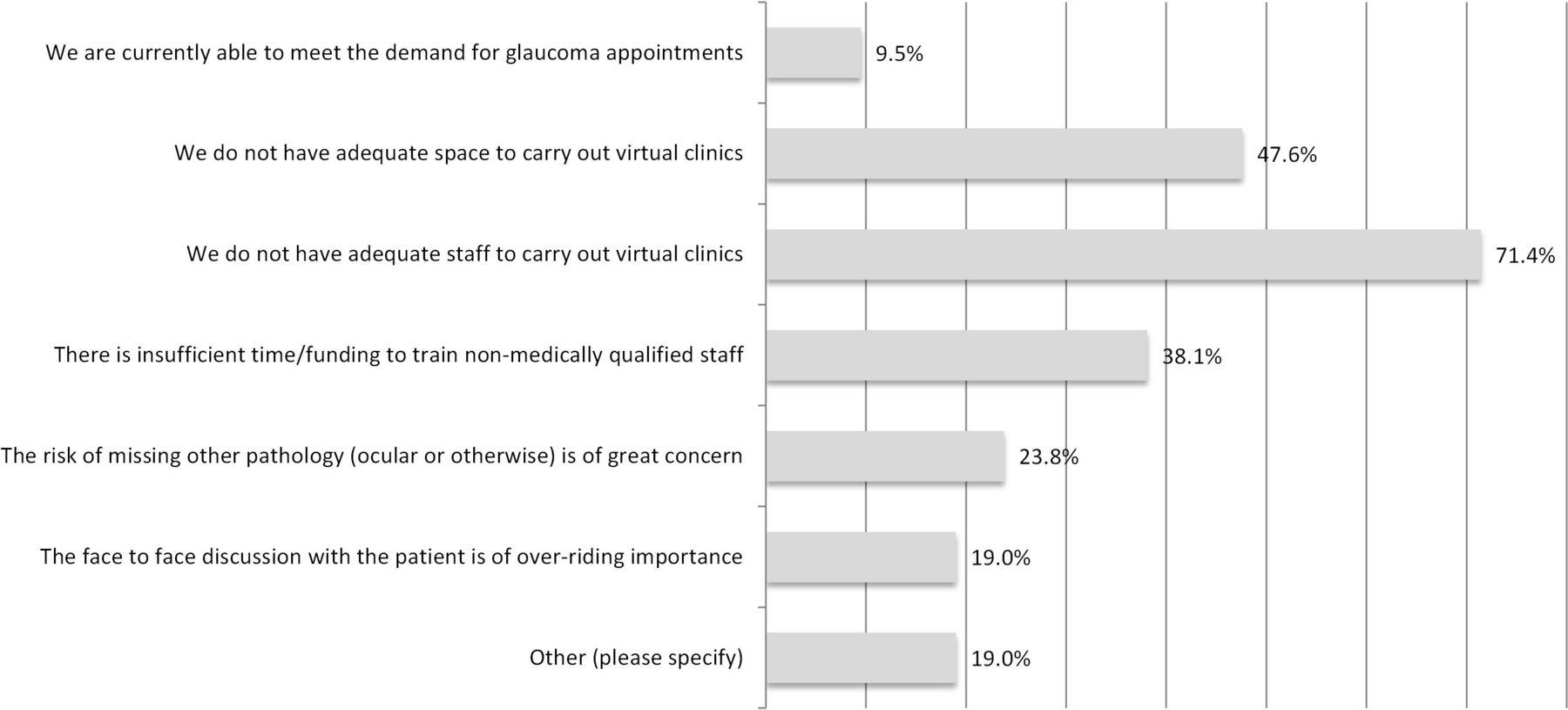
Clinical/glaucoma leads’ reasons for not running glaucoma virtual clinics (n=21). Respondents were asked to provide reasons if they were not running glaucoma virtual clinics. They were given a series of fixed responses as well as the option to specify any other specific reasons if not listed in the survey.
Inclusion criteria for glaucoma virtual clinics
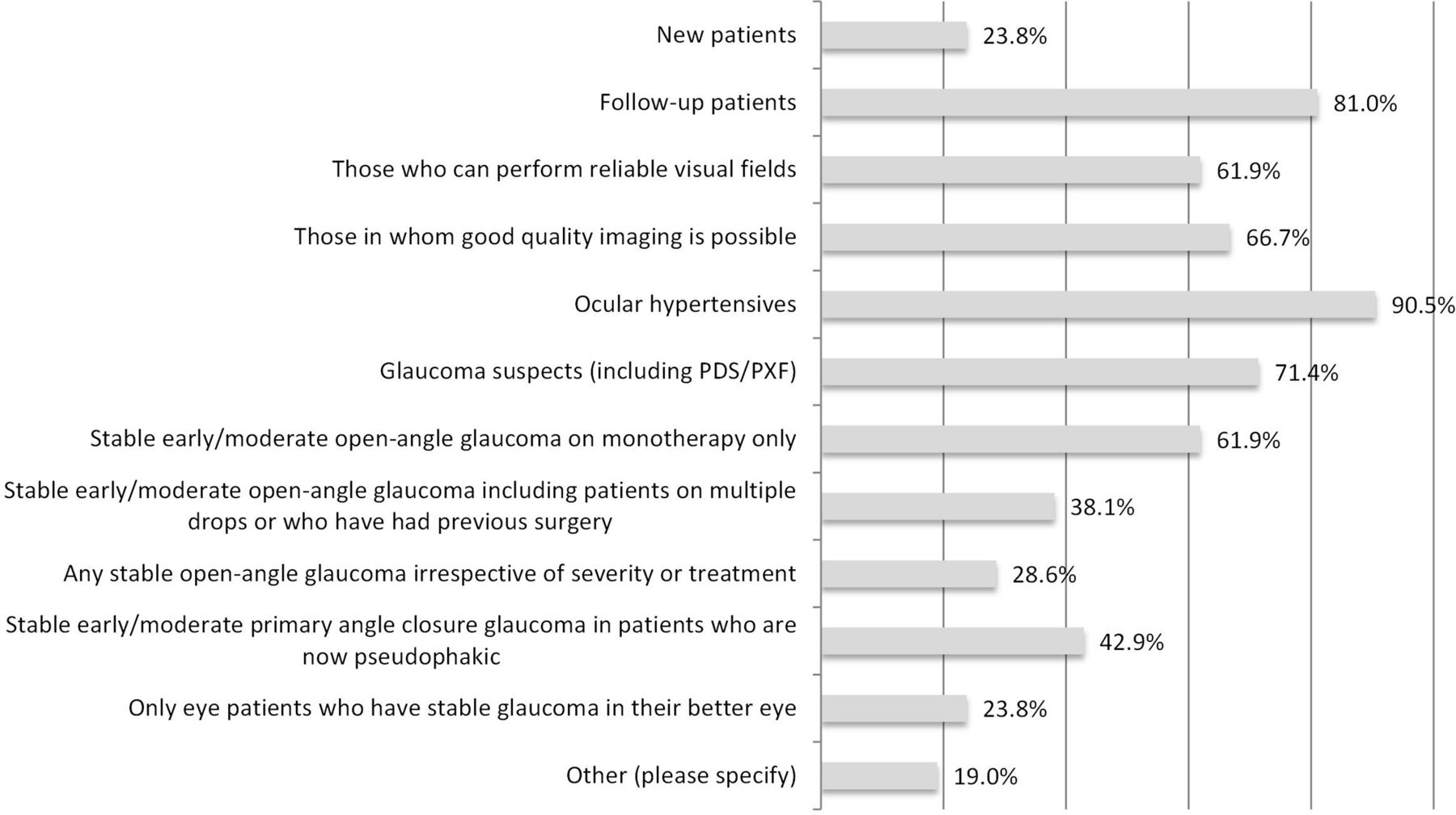
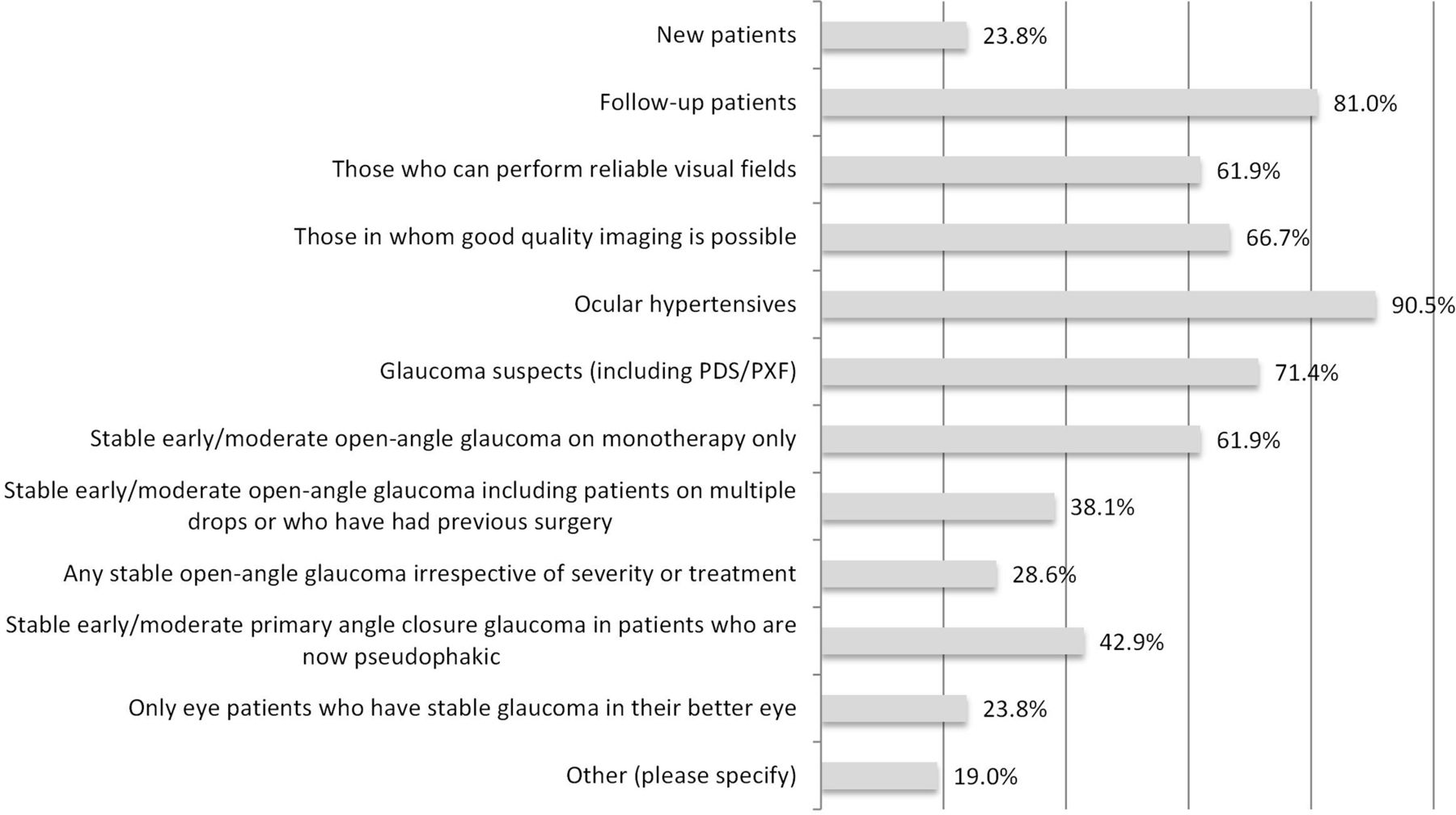
Of the 21 respondents using glaucoma virtual clinics, 14 (66.7%) used them to solely to review follow-up patients and 2 (9.5%) just to assess new patients. There were five respondents (23.8%) that used them for both. Thirteen out of 21 respondents (61.9%) only included patients who were able to perform reliable visual fields and 14 out of 21 respondents (66.7%) stipulated that good-quality imaging was required for inclusion into their glaucoma virtual clinics. The majority of those running virtual clinics used this model of care for ‘lower risk’ patients such as ocular hypertensives (19/21 respondents; 90.5%), GSs (15/21 respondents; 71.4%) and those with stable early/moderate open angle glaucoma on monotherapy (13/21 respondents; 61.9%). However, 6 out of 21 respondents (28.6%) reported that any patient with stable open-angle glaucoma could be included, regardless of treatment or severity, while just one respondent (4.8%) reported having used their glaucoma virtual clinic to review patients who had experienced undue delay in their scheduled outpatients’ appointments due to capacity issues. A single respondent (4.8%) commented that their glaucoma virtual clinic was for patients requiring a repeat visual field only. This data are summarised in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reported inclusion criteria used for patients seen in glaucoma virtual clinics (n=21). Respondents were asked to select as many inclusion criteria from the list provided for patients they would see in their glaucoma virtual clinic.
Glaucoma virtual clinic staffing and review
Technicians were the most common staff group reported to be working within glaucoma virtual clinics (20 out of 21 respondents; 95.2%), with just over half of all respondents (12/21 respondents; 57.1%) employing nurses and/or optometrists for data collection.
Electronic patient records were used by 11 out of 21 respondents (52.4%) in their glaucoma virtual clinics, with paper notes being used by four respondents (19.0%) and six respondents (28.6%) using a combination of the two. The vast majority of respondents who had implemented glaucoma virtual clinics used consultant ophthalmologists to review the results (20/21 respondents; 95.2%), 12 of which (57.1%) reported that virtual review was exclusively undertaken by consultant ophthalmologists in their unit. There were five respondents (23.8%) using optometrists with specialist qualifications in glaucoma to review results, and one service (4.8%) where results were exclusively reviewed by an optometrist.
Discussion
To date, there has been little evidence about how widespread the use of the virtual clinic model has become in caring for patients with glaucoma. Within our response rate of 45.7%, our survey estimates that 50.0% of UK HES units in NHS Trusts are currently using glaucoma virtual clinics, with a further 21.4% planning to introduce such a service. This response rate and estimate of virtual clinic adoption is very comparable to the recent figures determined by the Royal College of Ophthalmologists’ The Way Forward document for glaucoma,8 where 46.2% of glaucoma leads (24/52 respondents) had established glaucoma virtual clinic services.
Some researchers have described how different models of care can be provided using a glaucoma virtual clinic. Kotecha et al 9 described developing and implementing a virtual clinic for existing patients with glaucoma at Moorfields Eye Hospital in London, while Trikha et al 6 described using glaucoma virtual clinics for a glaucoma referral refinement scheme. As might be expected, our survey shows that most units implement virtual clinics to manage follow-up patients (81.0%), although a significant proportion of respondents (23.8%) were using the virtual clinic model to assess new patients.
In November 2016, the Royal College of Ophthalmologists released their Standards for Virtual Clinics in Glaucoma Care in the NHS Hospital Eye Service.10 This document aimed to define the minimum standards for the development and implementation of virtual clinics for glaucoma management in the secondary care setting and was produced by consensus from an expert panel. The document provides recommendations on patient suitability for virtual clinic monitoring, test procedures and processes, staffing, data collection and governance. The panel recommended that patients with ocular hypertension, suspected open angle glaucoma, or early or moderate glaucoma (open angle or pseudophakic patients with a history of angle closure) in the worse eye may be suitable for this type of clinic model. Our survey findings suggest that most respondents were already working within these recommendations, with 90.5% using virtual clinics to assess patients with ocular hypertension and 71.4% assessing glaucoma suspects. However, 28.6% of respondents included patients at any stage of disease, provided their condition was deemed to be ‘stable’ and one respondent reported using glaucoma virtual clinics for complex patients for intermittent follow-up appointments to avoid undue delays due to capacity issues within the service. The ‘Standards’ do allow for Consultant discretion in deciding on whom to refer to a glaucoma virtual clinic, although they do recommend excluding patients who have non-glaucomatous pathology. This recommendation is echoed by some survey respondents not planning on setting up a glaucoma virtual clinic, with 23.8% stating concern about missed pathology being a factor in their decision not to develop such clinics. Despite these concerns, the most common reasons stated for not establishing a glaucoma virtual clinic actually related to staffing (71.4%), insufficient space (47.6%), or time and funding to train staff (38.1%) to work within a glaucoma virtual clinic service. There were some concerns that face-to-face contact with patients was of overriding importance, with 19.0% respondents reporting this as a factor in deciding not to set up a glaucoma virtual clinic.
The standards panel also recommended that the virtual clinic should be led by a consultant ophthalmologist and that the glaucoma reviewer for this service should be a glaucoma clinician working within the secondary care team to whom the patient’s referring consultant is happy to delegate the role. Our survey showed all respondents using virtual clinics were exclusively using either consultant ophthalmologists and/or doctors/optometrists with specialist experience or qualifications in glaucoma.
The results of this survey show that consultant ophthalmologists perceive patients to be satisfied with the virtual model of clinical care, where 81.0% of clinical leads considered that patients’ perception of acceptability of glaucoma virtual clinics was at least similar to standard care and 52.4% rating virtual care as good or very good. Previous work has been undertaken on patients’ experiences in glaucoma virtual clinics, including that by Kotecha et al 11 and Court and Austin.12 In Kotecha et al’s study group, trust in the patient–provider relationship emerged as a key theme in patients’ acceptance of not being seen in a traditional doctor-delivered service. Patients who were well informed regarding their glaucoma status and at low risk of progression to sight loss were more accepting of being seen within a glaucoma virtual clinic. The research by Court and Austin showed their patient group had a mean satisfaction score of 4.3/5 in all areas surveyed. Virtual clinic patients’ understanding of their condition was very good and there was no evidence to support inferior knowledge or self-perceived understanding compared with standard clinic patients. Further work is necessary to fully understand patients’ experiences and perceptions of glaucoma virtual clinics.
Conclusions
This survey has determined that glaucoma virtual clinics are employed by a large proportion of HES units, with many others seeking to develop such services. Clinical leads largely rate efficiency, patient safety and the perception of patients’ acceptability to be at least equivalent to standard care. A paper by Clarke et al 13 published in 2016 showed agreement that glaucoma virtual clinics are safe, with misclassification events at just 1.9%. The glaucoma virtual clinics standards panel’s recommendations appear to be being adopted by most units implementing glaucoma virtual clinics. The recently published ‘Way Forward’ Document highlights some familiar barriers to use of glaucoma virtual clinics, raising clinicians’ concerns surrounding taking away the human, face-to-face element of decision-making.8 However, our survey also indicates that commonly reported barriers for clinicians relate to practical issues including having insufficient time, funding, staffing or space resources to establish and run virtual clinics. Interestingly, those working in acute trusts or major teaching hospitals were much more likely to have managed to overcome these barriers to set up a glaucoma virtual clinic. Despite the publication of some qualitative work on patients’ perceptions, there has been limited qualitative work in this field. While Kotecha et al 11 and Court and Austin’s12 studies have shown that patients are accepting of virtual clinics under certain provisos, these studies involved patients from a mainly Caucasian population with low-risk eye disease. Further qualitative research is necessary to understand more about both different patient groups and clinicians’ experiences and perceptions of virtual glaucoma clinics, to further inform approaches to this model of care.
Acknowledgments
The authors are grateful to Miss Fiona Spencer FRCOphth for her advice and to Mr Barney Foot of the Royal College of Ophthalmologists for his support in applying for College approval for the undertaking of this survey of clinical lead members.
Footnotes
Contributors PJGG is first author, who planned the study, collected the data and prepared this paper. JRM planned the study, collected the data and reviewed this paper. LA reviewed and contributed to the content of this paper. HW reviewed and contributed to the content of this paper. PGDS reviewed and contributed to the content of this paper. RAH planned the study, collected the data, reviewed and contributed to the content of this paper.
Funding This study was funded by the International Glaucoma Association.
Competing interests PGDS provides independent consultancy service to Newmedica. All other authors have no relevant conflict of interest declarations.
Provenance and peer review Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.