Article Text

Abstract
Purpose To investigate the association between baseline retinal microstructures observed with spectral-domain optical coherence tomography (OCT) and the need for early intervention in central serous chorioretinopathy (CSC).
Methods Cases of acute CSC from July 2011 to December 2014 were retrospectively reviewed. OCT images were further classified using six parameters: foveal serous retinal detachment; pigment epithelial detachment; fibrinous exudates in the subretinal space; retinal pigment epithelium bumps; thickened outer retinal layer and hyper-reflective dots in the intraretinal and/or subretinal layer. Correlation among these parameters and the need for intervention was analysed. Receiver operating characteristic (ROC) curves were performed to identify the optimal number of parameters for prediction.
Results A total of 47 eyes from 47 patients were included. Among these, 25 eyes required treatment. The presence of subretinal hyper-reflective dots was the only OCT factor having significant association with the need for intervention. An ROC curve analysis revealed that the optimal cut-off value (Youden index) was achieved when combining subretinal hyper-reflective dots with aged ≥50 years and female sex for analysis (area under the curve, 0.735; Youden index: 0.425).
Conclusion The presence of subretinal/intraretinal hyper-reflective dots observed with OCT, female and aged ≥50 years might help predict the need for early intervention in acute CSC.
- central serous chorioretinopathy
- intervention
- optical coherence tomography (OCT)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
Acute central serous chorioretinopathy (CSC) is generally a self-limiting disease; however, some patients experience poorer visual outcomes. This study used spectral-domain optical coherence tomography (OCT) to investigate the correlation of its features with the need for intervention in acute CSC. The presence of hyper-reflective dots observed with OCT, female, and aged ≥50 years might help predict the need for early intervention in acute CSC.
Introduction
Idiopathic central serous chorioretinopathy (CSC) is characterised by neurosensory retinal detachment (RD) retinal pigment epithelial (RPE) detachment that are most often confined to the macula. The hallmark of RD observed in CSC caused by choroidal vascular hyperpermeability can be visualised using indocyanine green angiography (ICGA), while focal leakage at the RPE level can be observed using fluorescein angiography (FA).1
With the advent of optical coherence tomography (OCT), it is now possible for clinicians to obtain high-resolution cross-sectional images and to evaluate microstructural changes and retinal abnormalities in a non-invasive fashion. Various reports on OCT have shown the features of CSC, including neurosensory RD, pigment epithelial detachment (PED), fibrinous exudates, RPE bumps, thickened outer retinal layer, hyper-reflective dots in the intraretinal layer and/or subretinal layer and a disrupted inner/outer segment (IS/OS) line.1–3 Some of these pathological changes helped identify stage and predict prognosis.1 3
Acute CSC is generally a self-limiting disease with a favourable prognosis; however, some patients experience a chronic condition that results in poorer visual outcomes. Therefore, during the early stages of the disease, identification of certain groups that might need early intervention is important. This study used spectral-domain (SD)-OCT to investigate the correlation of morphological OCT features with the need for intervention in acute CSC. A possible relationship between gender and age was also investigated.
Methods
This study was designed to be a retrospective, observational and cross-sectional case series. A retrospective chart review was conducted for patients who were diagnosed with acute CSC from July 2011 to December 2014 at Kaohsiung Veterans General Hospital. The institutional review board and ethics committee of Kaohsiung Veterans General Hospital approved this study, which adhered to the tenets of the Declaration of Helsinki.
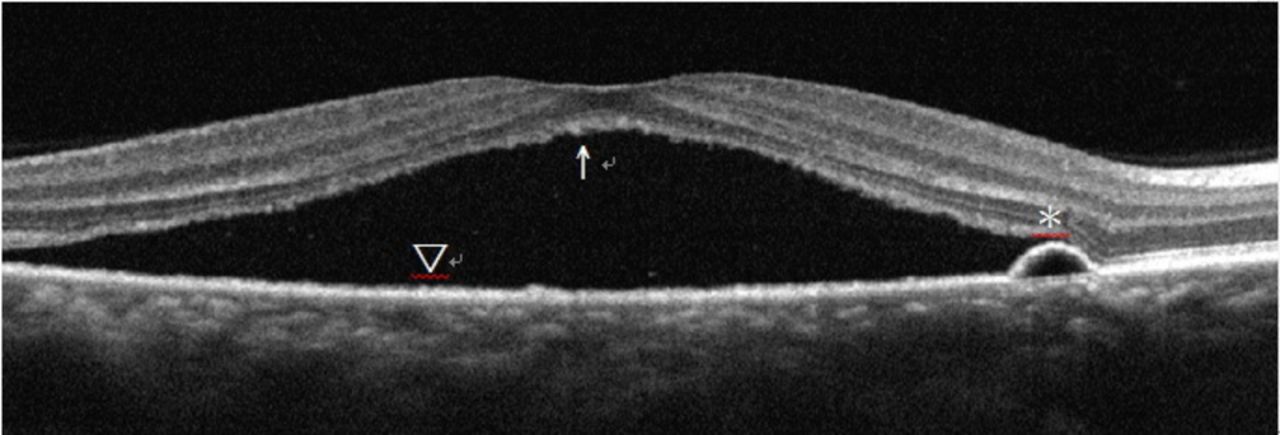
Idiopathic CSC was diagnosed based on the presence of a serous detachment of the neurosensory retina involving the macula that was confirmed using one of the following: SD-OCT, leakage at the RPE level using FA or choroidal hyperpermeability with ICGA. ICGA was not routinely performed but was used in cases where severe pachychoroid pigment epitheliopathy was suspected. None of them showed findings compatible with definitive PCV. Acute CSC was defined as the onset of subjective symptoms such as blurred vision, metamorphopsia, chromatopsia or micropsia that had occurred within the past 6 weeks. Recorded data included age, sex, disease onset duration, vision, biomicroscopic examinations, OCT images, fundus pictures and FA or ICGA if eligible. All OCT images were obtained through a dilated pupil using SD-OCT (Optovue, RTVue-CAM, Optovue, Fremont, California, USA or Heidelberg Spectralis OCT, Heidelberg Engineering, Heidelberg, Germany). These images were further classified using six parameters: foveal serous RD, PED, fibrinous exudates in the subretinal space, RPE bumps, thickened outer retina layer and hyper-reflective dots in the intraretinal and/or subretinal layer. Schematic representations are shown in figures 1, 2. Patients whose CSC development had strong association with steroid were excluded. These patients often have underlying diseases that could not tolerate discontinuation of systemic steroid treatment. Inclusion of such cases would complicate the evaluation as to whether it was the course of the disease or the effect of systemic steroid that contributed to the conditions observed. Eyes with other retinal abnormalities such as neovascular maculopathy (ie, polypoidal choroidal vasculopathy, age-related macular degeneration, idiopathic choroidal neovascularisation or retinal vascular diseases), intraocular inflammation and a posterior segmental tumour, and patients who were not followed-up for at least 3 months or had incomplete data were excluded. Observation and lifestyle modification were first recommended. Additional interventions were considered under the following rationales: CSC with persistent or increased macular subretinal fluid for 3 months or longer during follow-up or progressively decreased visual acuity. These patients were given further interventions, which included intravitreal injection of antivascular endothelial growth factor, photodynamic therapy or laser.

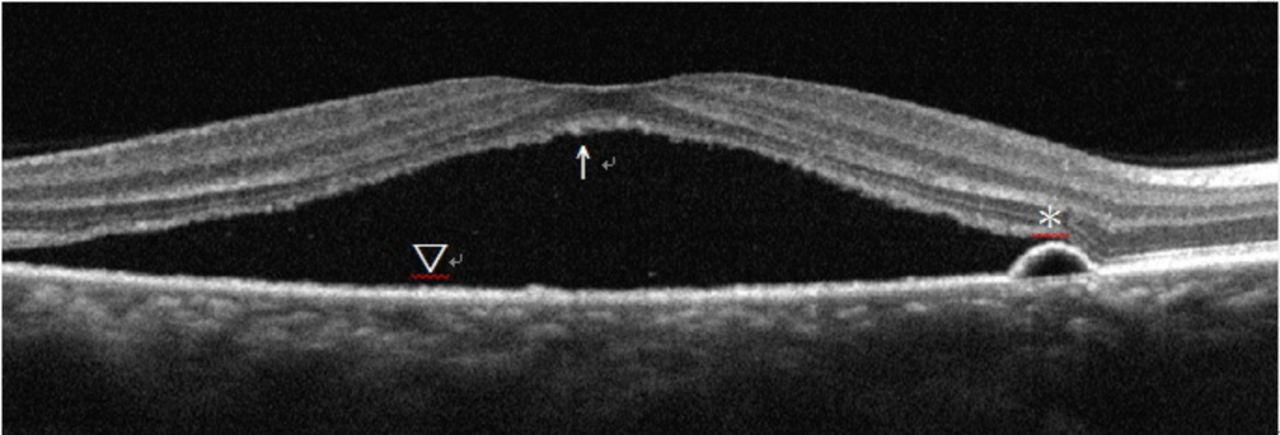
Schematic diagrams of the six optical coherence tomography parameters. Arrow: hyper-reflective dots. Asterisk: thickened outer retina. Triangular arrowhead: fibrin. Arrowhead: pigment epithelial detachment. Note that the intraretinal bright dots are mostly observed in the outer layer of the neurosensory retina.
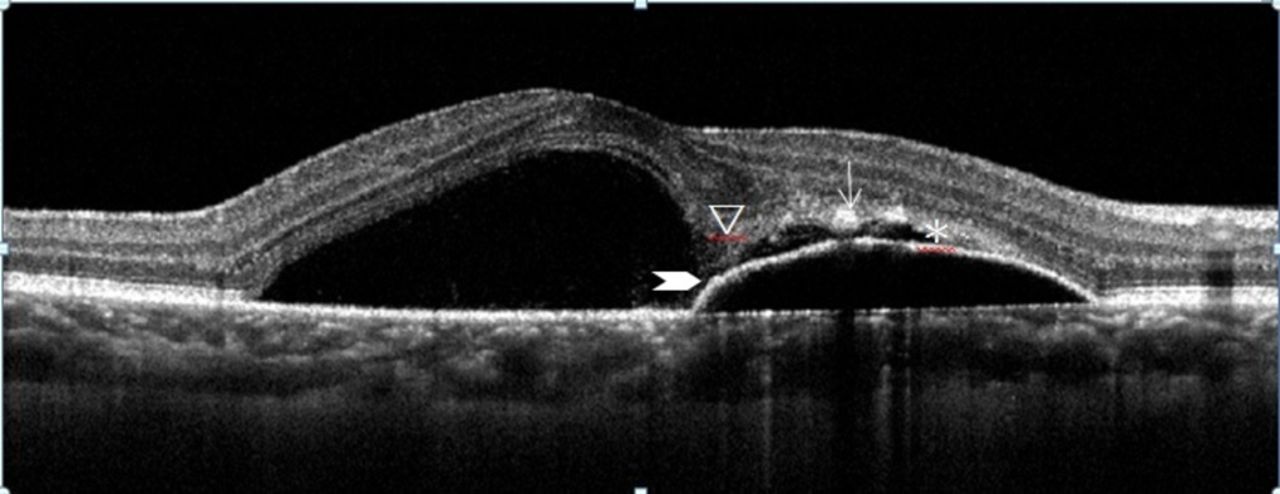
Schematic diagram of the six optical coherence tomography parameters. Arrow: hyper-reflective dots. Asterisk: pigment epithelial detachment. Arrowhead: retinal pigment epithelial bumps.
Statistical analysis
Statistical analysis was performed using SPSS for Windows (V.20.0 software package; SPSS, Chicago, Illinois, USA). Differences in age, gender and SD-OCT characteristics between the observational group and treatment-needed group were compared using independent t-test and χ2 test. Multiple logistic regression analyses with forward selection were performed to determine significant prediction variables. Each patient was coded on the basis of presence of OCT characteristics, age and gender, to which each of the six OCT characteristics, aged ≥50 years and female, were scored an equal weight of 1 point. For the presence of each of the OCT characteristics, 1 point was coded and summed up. Idiopathic CSC is generally self-limiting and is more common in men between 20 and 45 years of age4 5; hence, it was hypothesised that older female might warrant more intense monitoring. Therefore, aged ≥50 years and female were each scored 1 point. The six OCT characteristics, as well as sex and age, were added stepwise as test variables in different receiver operating characteristic (ROC) analyses, and four model test variables A–D were thus developed. Model A represents the sum of the six OCT characteristics. Model B represents model A plus ‘hyper-reflective dots in the intraretinal layer and/or subretinal layer’. ‘Hyper-reflective dots in the intraretinal layer and/or subretinal layer’ was specifically selected because it was the only significant variable among the six OCT characteristics in χ2 test and multiple logistic regression test with forward selection. Model C represents model B plus sex, and model D represents model C plus age. Youden index was used as an index for the optimal cut-off of test variables. Finally, the corresponding sensitivity and specificity were calculated. Area under the ROC curve was employed to assess the discriminatory ability for intervention using a differential diagnosis strategy according to SD-OCT findings. A p value of <0.05 was considered to be statistically significant.
Results
Data were collected from 47 eyes of 47 patients, including 35 males and 12 females. The clinical characteristics and reasons for intervention were listed in online supplementary appendix 1. Twenty-five patients required treatment according to retinal specialists. The mean age of the observational group and treatment-needed group was 44.5±7.70 (range, 30–58 years) and 46.88±8.09 (range, 33–66 years), respectively, and there was no significant difference in mean age between the two groups (p=0.309, independent t-test). There were 18 male and 4 female patients in the observational group, 17 male and 8 female patients in the treatment-needed group, with no significant difference in sex between the two groups (p=0.33, χ2 test). At their initial visits, the mean time from the onset of subjective symptoms in patients with acute CSC was 16.27±11.50 days (range, 3–42 days) in the observational group and 23.48±14 days (range, 4–42 days) in the treatment-needed group, indicating no significant difference in mean disease onset duration between the two groups (p=0.096, independent t-test) (table 1).
Supplementary file 1
Comparison of demographic and OCT features between observational and treatment groups
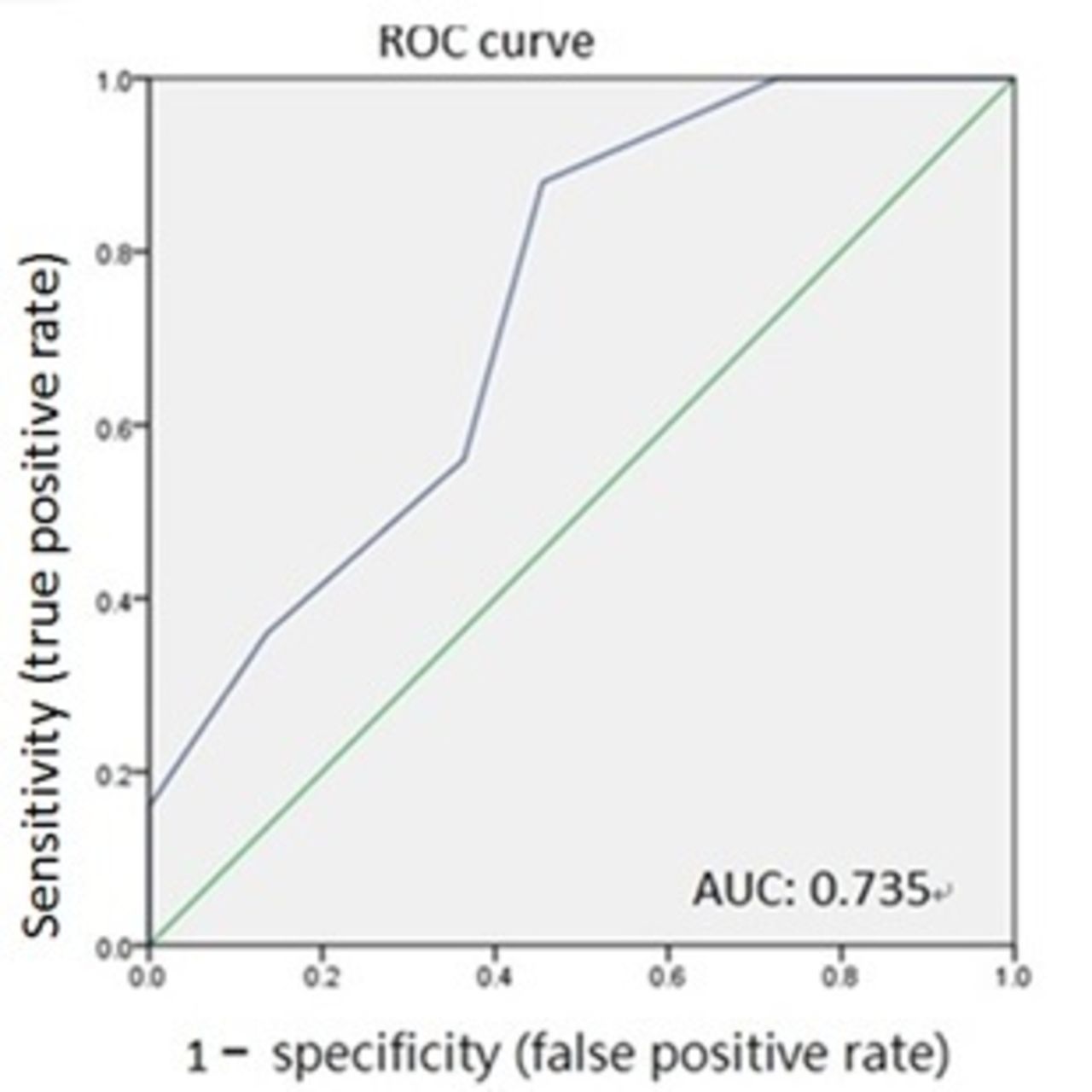
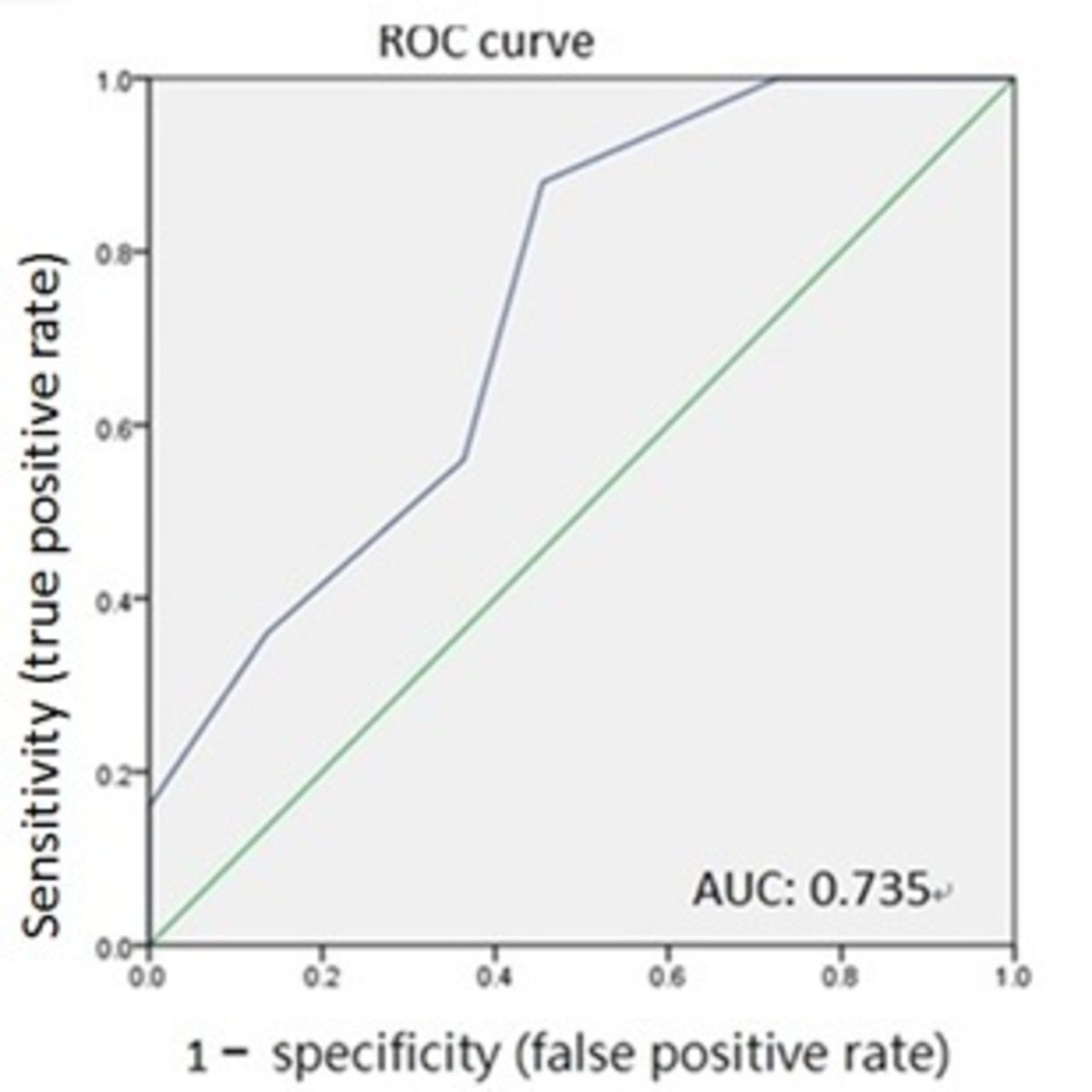
Comparison of age, sex and the six OCT characteristic features between the observational and treatment-needed groups is shown in table 1. Of the eight parameters, only 'hyper-reflective dots in the intraretinal layer and/or subretinal layer' demonstrated significant association with the need for treatment (p=0.031, χ2 test=0.035, multiple logistic regression with forward selection). Therefore, 'hyper-reflective dots in the intraretinal layer and/or subretinal layer' was added into the model for further analysis. In order to obtain the best predictor, four models were generated with operative variables being added stepwise. In model B, an ROC curve analysis was plotted and revealed that the optimal cut-off value (Youden index) was achieved if the total score was 4 points. In other words, 'hyper-reflective dots in the intraretinal layer and/or subretinal layer' plus presence of two other OCT characteristics, or four out of five remaining OCT characteristics besides 'hyper-reflective dots in the intraretinal layer and/or subretinal layer' achieved Youden index of 0.391 (AUC, 0.699; specificity, 0.59; sensitivity, 0.80) when only OCT images were considered. Adding both aged ≥ 50 years and female sex into the model (model D) improved the overall accuracy (AUC, 0.735; specificity, 0.55; sensitivity, 0.88) for predicting the need for intervention (figures 3, 4 table 2).
Diagnostic index of four models with different test variables
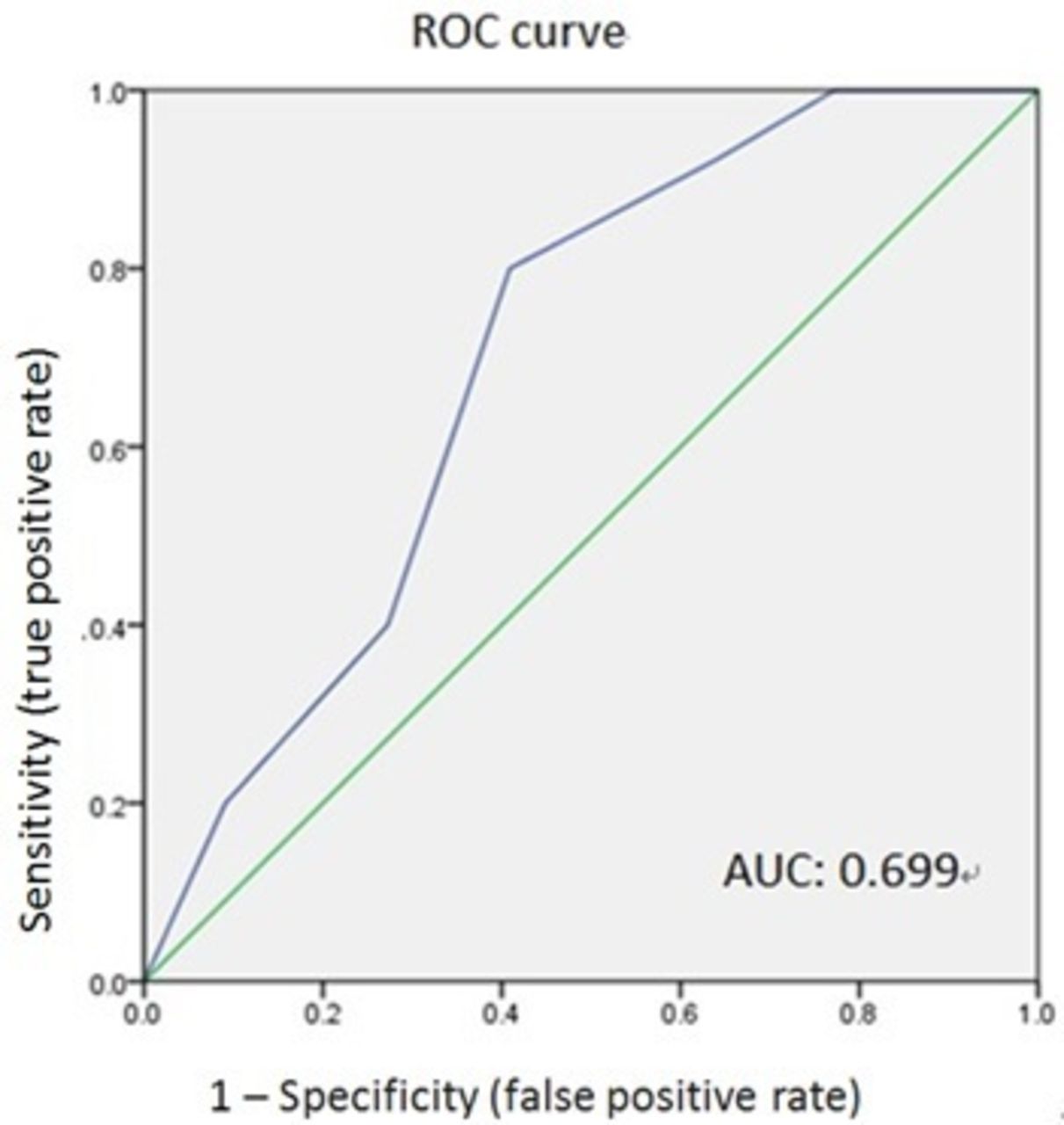
Receiver operating characteristic (ROC) curve and area under the curve (AUC) of model B: the total score of ‘the presence of six optical coherence tomography (OCT) characteristics’ plus ‘hyper-reflective dots’. The optimal cut-off value (Youden index) was achieved if subretinal/intraretinal hyper-reflective dots plus two other OCT parameters were present when only OCT images were considered (AUC, 0.699; specificity, 0.59; sensitivity, 0.80). (Note: each OCT characteristic: 1 point if present; otherwise, 0 point.)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curve and area under the curve (AUC) of model D: the total score of ‘the presence of six optical coherence tomography (OCT) characteristics’, ‘hyper-reflective dots’, ‘female’, plus ‘aged 50 years and older’. The optimal cut-off value (Youden index) had improved (AUC, 0.735; specificity, 0.54; sensitivity, 0.88). (Note: each OCT characteristic: 1 point if present; otherwise, 0 point; female: 1 point, male: 0 point; aged ≥50 years: 1 point, aged <50 years: 0 point.)
Discussion
Microstructural changes in idiopathic CSC have attracted much interest in recent years. Morphological changes observed with OCT have provided an objective method for estimating disease chronicity.1 Certain OCT morphologies, such as bullous subretinal fluid; posterior dragging; thickened posterior surface of a detached retina; RPE bumps; thickened outer retinal layer as well as subretinal and/or intraretinal hyper-reflective dots, have shown to be characteristics of idiopathic CSC during the acute stage.1 2 6 7
In the present series, the overall incidence of hyper-reflective dots was 57.4%, which was comparable with previous results obtained by Yalcinbayir et al 2 (66%) and Maruko et al 8 (65%). It was the only factor showing significant correlation with the need for intervention among the six baseline retinal microstructures observed with OCT in our study. The presence of intraretinal and/or subretinal hyper-reflective dots in CSC has been studied and shown to be related to poor visual outcomes.2 7–10 Evidence in medical literature has indicated that hyper-reflective dots may comprise macrophages and disintegrated outer photoreceptor remnants and that intraretinal deposits may accumulate secondary to the inability of RPE cells to pump highly proteinaceous subretinal fluid (SRF) from the intraretinal spaces to the subretinal spaces.2 9–11 These dot-like precipitates were seen in subretinal spaces and in intraretinal spaces.11 The appearance of intraretinal/subretinal hyper-reflective areas could be seen as early as the same day of symptom onset, followed by progression to the deeper retinal layer.10 According to the known importance of the presence of intraretinal and/or subretinal hyper-reflective dots, the current results offer the first evidence on its significance in predicting the need for early intervention.
CSC has been thought to be a disease primarily affecting men early in life, with age at diagnosis ranging from 20 to 45 years.4 5 Furthermore, a wide variety of systemic factors are associated with CSC.12 This study found that aged ≥50 years and female sex significantly improved the prediction of sensitivity to 88%. Neither old age nor female sex had been reported as a predisposing factor for CSC development. In previous reports, initial visual acuity and symptom duration were shown to be predictors of poorer visual prognosis.13 The present findings suggested that females aged ≥50 years were more likely to need early intervention and thus require more frequent monitoring.
As shown in the current results, the AUC reached 0.735 by setting different cut-off points, suggesting that SD-OCT was useful in predicting the need for treatment. OCT is a well-known non-invasive tool for monitoring changes in retinal conditions in various retinal diseases. The combination of hyper-reflective dots, aged ≥50 years and female sex demonstrated a specificity of 54% and a high sensitivity of 88% and a satisfactory Youden index of 0.425. Considering the above combination offers a practical and convenient method in clinical setting to assess whether observation alone is adequate or whether more frequent monitoring is mandated.
Although acute CSC is a self-limiting disease, long-lasting CSC in chronic or recurrent cases does occur, with increased photoreceptor damage and functional loss. The longer the duration, the more severe damage is expected. Although no consensus exists regarding the most suitable treatment, several treatment modalities have been reported with an acceptable effect.14 If a specific group requiring early intervention could be identified at an early stage, additional preventable damage could be avoided using more frequent monitoring and earlier treatment. This study highlights that SD-OCT findings could aid in deciding whether more frequent monitoring at the time of a patient’s first examination is needed to determine if an earlier treatment modality should be initiated. In conclusion, the presence of subretinal/intraretinal hyper-reflective dots observed with OCT, female sex and aged ≥50 years in acute CSC might help predict the need for early intervention.
The current study was limited by its cross-sectional design and small sample size. Additional longitudinal studies with more cases and longer follow-up periods are needed to gain more in-depth understanding of acute CSC.
Reference
Footnotes
Contributors WYL participated in acquisition, analysis and interpretation of data and also drafted the manuscript. TTW participated in the acquisition of data. CLT and HSL participated in the analysis and interpretation of data. SJS conceived of and coordinated the study, and also revised critically the manuscript. All authors read and approved the final manuscript.
Competing interests None declared.
Ethics approval Ethical approval was obtained from the local ethics committee of Kaohsiung Veterans General Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data from the study are being published.