Article Text

Abstract
Aim The aim of this study was to determine the level of awareness and knowledge of glaucoma and the proportion of people with glaucoma among participants of a 1-day urban eye outreach programme.
Methods The study was a cross-sectional survey. Data, collected by means of a structured questionnaire, included participants' demographic details, and awareness, knowledge and ocular status as regards glaucoma. Publicity for the outreach was created through the mass media (radio stations and television), churches, handbills, posters and different hospital staff. Data analysis was by Statistical Package for Social SciencesV.20.0. Associations between participants' demographic and other details were tested using Pearson's χ2 test, and a p value of <0.05 was considered significant.
Results Four hundred and seventy-eight (93.2%) of the 513 people in attendance were eligible and consented to participate. Awareness, knowledge and proportion of people with glaucoma in the study population were 65.5%, 36.8% and 14.5%, respectively. Awareness was significantly associated with attainment of some formal education, awareness of a positive family history, and having had an eye check prior to the outreach. The mass media was the most common information source. Good knowledge level was significantly associated with higher educational attainment and occupation, whereas proportion of people with glaucoma was significantly associated with increasing age.
Conclusion Improving awareness with suitable content for the target population through effective means such as the mass media may be a veritable first step in combating blindness from glaucoma.
- Glaucoma
- awareness
- knowledge
- Southeast Nigeria
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Glaucoma is the leading cause of irreversible blindness globally.
Poor awareness and late presentation often militate against effective management of the condition.
What are the new findings?
Awareness does not invariably translate to adequate knowledge of glaucoma.
The mass media is a potentially effective tool for disseminating information about glaucoma.
How might these results change the focus of research or clinical practice?
For awareness efforts to be efficient, their contents have to be tailored to suit the needs of the target audience.
Screening programmes are important in creating awareness and detecting glaucoma suspects and cases , and may help alleviate the problem of late presentation.
Introduction
Glaucoma is a group of diseases that cause structural damage and visual field dysfunction, leading to progressive and irreversible vision loss.1 It is the second leading cause of blindness globally, accounting for 8% of blindness.2 Open angle glaucoma is the predominant type in people of African descent, in whom it has an earlier onset and more aggressive progression.1 3
In Nigeria, the prevalence is 5.02% (95% CI 4.60% to 5.47%) in people aged 40 years and older, with open-angle glaucoma and angle closure glaucoma comprising 86% and 14% of cases, respectively.4 Secondary glaucoma accounts for 8% of cases.4
Open-angle glaucoma usually runs a symptomless but progressive course, affecting the peripheral vision first. Therefore, many affected remain undiagnosed, presenting only when the disease has progressed significantly to affect the central vision late in the disease process. Late presentation is therefore an important setback in glaucoma management.5–7 In a review of population-based studies by Quigley and Broman,8 the global rate of previous diagnosis of open-angle glaucoma was low at 26%, and even lower at 8% for developing countries. In Nigeria, the rate was 5.6%,4 and more than half of patients are blind in one or both eyes at presentation.5 9 10 Late presentation has been attributed to low level of awareness about glaucoma, especially in developing countries.7 11–14 Creating awareness about the disease, its insidious nature and the importance of early detection and treatment in preventing blindness is therefore key in glaucoma control.
There is currently no consensus on a precise and easily implemented screening test or strategy for glaucoma detection.15 Population screening has not been found to be cost-effective,16 and opportunistic case finding may miss a majority of those with glaucoma.17 Screening targeted at high-risk groups such as blacks and people with a positive family history in first degree relatives16 and incorporation of glaucoma screening into other eye screening programmes such as cataract screening programmes have been suggested as more feasible control strategies.18 19
A study in Ibadan, Nigeria, that evaluated the effectiveness of screening programmes in early detection of glaucoma18 revealed that patients referred from outreach screening programmes were more likely to present with mild to moderate diseases than their counterparts referred from other sources. Such screening programmes may therefore be invaluable in early detection of glaucoma and may serve as feasible means of improving public awareness of the condition. Evidence necessary for planning can also be generated by examining the demographic features and visual characteristics of patients attending such outreach programmes.
The aim of this study was to determine the level of awareness and knowledge of glaucoma and the proportion of people with glaucoma among participants of a glaucoma urban outreach exercise. To the best of our knowledge, this is the first report of such a study carried out on an urban outreach population in Southeast Nigeria. Igbos, the predominant ethnic group in this region, as well as urban dwellers, have the highest prevalence of glaucoma in the country.4 The findings provide important evidence for efficient planning of comprehensive glaucoma management in the region.
Materials and methods
The study was a cross-sectional survey of participants of a 1-day eye outreach programme in March 2015 in an urban area in Enugu State, Southeast Nigeria. The programme was widely publicised through the mass media (radio and television), church bulletins and announcements, and posters and announcements at eye clinics of the two tertiary-level eye hospitals in the study area. The programme took place in a field beside the premises of a popular church in the study area, whereas ocular examinations were carried out in an adjacent private eye hospital.
The study participants comprised all consenting participants of the programme aged 18 years or older. This age cut-off was chosen to ensure that participants would be able to answer the questions correctly. Trained facilitators collected data on the first aspect of a two-part structured questionnaire, whereas the second part was completed by ophthalmologists after ocular examination.
The primary outcomes of interest were awareness, knowledge and the proportion of people with glaucoma among participants. Awareness of glaucoma was assessed based on whether participants had heard about glaucoma prior to the programme. Knowledge was assessed using eight questions. A score was assigned to each question correctly answered. The level of knowledge was classified as ‘good’ (five or more correct answers) or ‘poor’ (less than five correct answers).
Participants then underwent visual assessments (visual acuity (VA), intraocular pressure measurement and funduscopy). Visual fields could not be assessed due to the logistic challenges of an outreach programme. All identified glaucoma cases and suspects were appropriately counselled and referred for further evaluation and management.
The following criteria, adapted from the International Society of Geographical and Epidemiological Ophthalmology definitions for glaucoma in prevalence surveys20 and the normative data for Nigeria,21 were used to determine the glaucoma status of participants:
Glaucoma cases
Glaucoma category 2 (structural damage, visual field not done): vertical cup–disc ratio (VCDR) >0.75 (99.5th percentile) or VCDR asymmetry >0.2 (99.5th percentile)
Glaucoma category 3 (no view of fundus and no visual field): VA <3/60+intraocular pressure (IOP) >28 mm Hg (99.5th percentile) OR VA <3/60+evidence of glaucoma filtering surgery or medical records showing visual glaucomatous morbidityGlaucoma category 1 (structural and typical visual field defect) was not included as visual fields were not assessed.
Glaucoma suspects
Disc suspects: VCDR >0.7 (97.5th percentile) or VCDR asymmetry >0.1 (97.5th percentile)
IOP suspect: IOP >20 mm Hg (97.5th percentile)
IOP + disc suspect: meets both disc suspect and IOP suspect criteria
Data were analysed using IBM Statistical Package for Social Sciences (SPSS) version V.20. For ease of analysis, the ages of participants were presented and analysed in intervals of 10, except for people aged 18–29 years and >70 years. Means and SD were calculated for quantitative variables, whereas frequencies and percentages were calculated for qualitative variables. The relationships between demographic and other features of participants, and awareness, knowledge and proportion of people with glaucoma were explored using Pearson's Chi-squareχ2 test for categorical and dichotomous variables. p Values <0.05 were considered statistically significant.
The study abided by the guidelines of the Declaration of Helsinki and ethical approval was granted by the Ethics Review Committee of the Enugu State University of Science and Technology Teaching Hospital, Parklane, Enugu, Nigeria. Informed consent was obtained from all participants prior to their inclusion in the study and was not a prerequisite to being part of the outreach programme.
Results
Of the 513 participants who attended the programme, 478 (93.2%) people were aged 18 years and older and consented to participate in the study. All analyses were based on these 478 eligible participants except analyses of proportion of people with glaucoma that involved only people who were completely examined (n=469). Mean age was 50 (SD± 15.4) years with a range of 18–92 years. Participants were predominantly of the Igbo ethnic group (n=474/478, 99.2%). There were slightly more men than women (1.2:1). Two hundred and eighty-nine (60.8%) people came because of an eye problem, whereas the rest came for routine eye checks. The mass media was the most common source of information about the outreach (n=361/478, 75.5%), followed by information from family and friends (n=62/478, 13%). The sociodemographic characteristics of participants are shown in table 1.
Sociodemographic characteristics of eligible participants at the eye outreach programme
Business/self-employed people were the most common occupational group (n=124/478, 25.9%).
Two-hundred and twenty-two (46.4%) participants had their eyes checked for the first time at the outreach programme. Among those who had had a previous eye check (n=256/478, 53.6%), 140 (54.7%) had had their eyes checked within the preceding 1 year. Two hundred and eighty-nine (60.5%) people came because they had eye complaints, and 365 (77%) said they would still have come even if they had to pay to have their eyes checked.
Awareness about glaucoma
Two-hundred and ninety-three (61.3%, 95% CI 56.3% to 65.5%) participants had heard of glaucoma prior to the outreach. The mass media was the most common source of information (n=169, 57.7%), followed by information from a health worker (n=77, 26.3%) and from family members or friends (n=36, 12.4%).
Only 47 (9.8%, 95% CI 7.3% to 12.6%) people were sure of a positive family history of glaucoma, of which 39 (83%) were first-degree relatives (28 parents, 9 siblings and 2 children).
The relationship between awareness and demographic and other features of participants are shown in table 2.
Determinants of awareness of glaucoma among the study participants
Awareness of glaucoma was strongly associated with higher levels of education, awareness of a positive family history of glaucoma and having had an eye check prior to the outreach programme. People who had primary education or greater were more likely to be aware of glaucoma than people who had no formal education (Xχ2 (4, n=478)=26.4, p<0.001). All the patients who were aware of a positive family history of glaucoma (n=47) had heard of glaucoma before the outreach (χ2 (1, n=478)=32.912, p<0.001). Awareness of glaucoma was higher in people who had had a previous eye check (n=188/256, 73.4%) than in people who were having their eyes checked for the first time (n=105/222, 47.3%) (χ2 (1, n=478)=34.245, p<0.001).
The mass media was the main source of information for both participants who had had previous eye checks (n=100/188, 53.2%) and those having their eyes checked for the first time (n=69 of 105, 65.7%) (χ2 (4, n=293)=10.231, p=0.037). However, 31.9% (60) of people with previous checks had heard through a health worker/hospital setting compared with 16.2% (17) of first timers who heard through the same source.
Knowledge about glaucoma
Participants who were aware of glaucoma (n=293/478, 61.3%) were questioned further to assess their knowledge about glaucoma using eight questions (figure 1). Questions asked bordered on effects, perceptions and management of glaucoma.

Responses to questions on knowledge about glaucoma.
Most people knew that glaucoma causes blindness (n=245/293, 83.6%) and that it can be managed by means of drugs (n=198/293, 67.6%) and surgery (n=187/293, 63.8%). One hundred and thirty-four (45.7%) people were unsure or said it was a spiritual problem or curse. More than a third (107/293, 36.5%) did not know that vision loss due to glaucoma is irreversible.
Knowledge was assessed using a knowledge score as described in the methodology. A ‘good’ knowledge score was recorded for 176 of the 293 people (60.1%, 95% CI 50.0% to 65.9%) that were aware of glaucoma. This accounts for 36.8% of the total study participants.
The relationship between knowledge score of participants and their demographic and other features are shown in table 3.
Determinants of knowledge of glaucoma among the study participants
Occupation and level of education were significantly associated with knowledge of glaucoma. There was a strong association between level of education and knowledge of glaucoma (χ2 (4, n=293)=22.640, p<0.001). The higher the level of education attained, the greater the percentage of people with ‘good’ knowledge, rising from 26.7% (n=4/15) in people with no formal education to >70% in people with tertiary education and higher. About three-quarters (n=11/15, 73.3%) of the people who had no formal education had poor knowledge of glaucoma.
A similar association was also noted for occupation and knowledge about glaucoma (χ2 (6, n=293)=17.409, p=0.008). The ‘farmer/labourer’ occupation group had by far the highest proportion of people with poor knowledge of glaucoma (n=32/51, 62.7%). They also had the highest proportion of people who had no formal education (20/43, 46.5%) or only primary education (42/111, 37.8%), and this was statistically significant (χ2 (24, n=478)=196.631, p<0.001).
Proportion of people with glaucoma
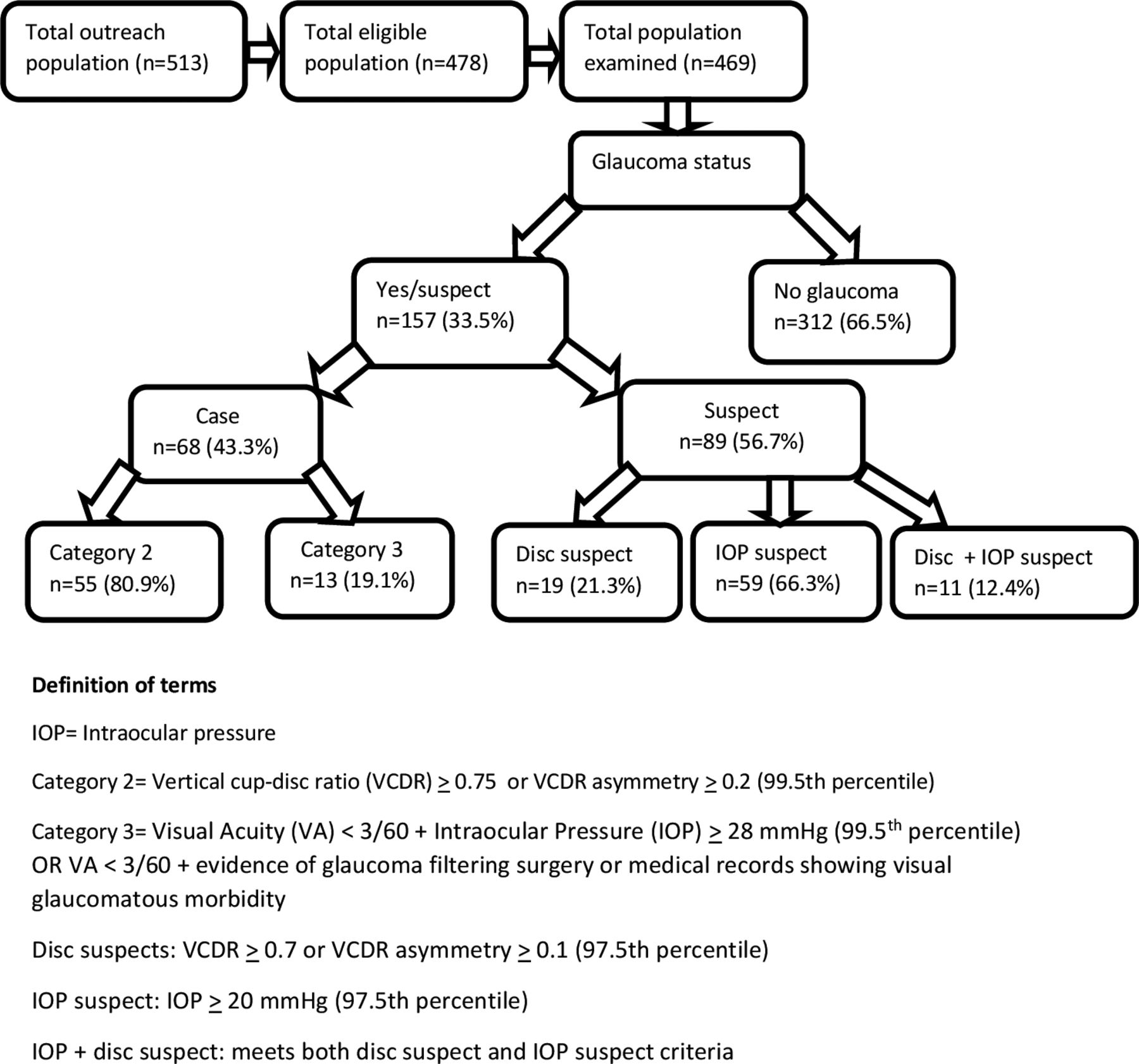
Of the 478 eligible participants, 469 (98.1%) underwent ophthalmic examination, whereas nine people left before they could be examined and were therefore excluded from the analysis of this section. The proportion of people with glaucoma in the study population was 14.5% (68/469, 95% CI 11.7% to 17.7%), affecting 38 (14.7%) men and 30 women (14.3%). The proportion increased significantly with increasing age from about 1.9% in people younger than 30 years to 25% in people 70 years and older (χ2 (5, n=469)=26.685, p<0.001).
Four hundred and forty-three (94.5%) of the 469 people examined said they did not have glaucoma, but 11.1% (49) of them had glaucoma on examination.
About a fifth (13/68, 19.1%) of glaucoma cases detected were blind with presenting VA <3/60 in the better eye. The diagnosis of glaucoma was not significantly associated with family history of the condition.Figure 2 shows the different categories of participants with respect to their glaucoma status.
{kind=link}
{kind=link}
Categories of participants with respect to their glaucoma status.
Discussion
Glaucoma is the leading cause of irreversible blindness in Nigeria,22 and poor awareness and late presentation are often major impediments to adequate management and prevention of blindness from the condition.
There was a generally high level of awareness (n=293/478, 61.3%) of glaucoma among participants in this study compared with other outreach-based studies. In Southwest Nigeria14 and Ethiopia,13 the levels of awareness were lower at 15.8% (n=41/259) and 2.4% (n=8/340), respectively. These studies were however carried out on rural populations. The level of awareness found in this study is more similar to levels reported in studies carried out among hospital and university staff in Nigeria of 68.6%23 and 46.8%,24 respectively. In a population-based study in urban Chennai, South India, awareness level was only 13.5% (n=1926).11
High awareness of glaucoma in this population may be attributed to accessibility to mass media, which was the major source of information about glaucoma in this study (n=168/291, 57.7%). A lot of awareness about glaucoma had been created in the study town in the preceding 5 years through the mass media especially the radio, with accompanying free eye screening exercises (such as that for this study) about three times a year. Although there is no published baseline study to which the results of this study population can be compared, results of studies in Ethiopia25 and of an Indian population in London26 indicate that awareness campaigns through the mass media can significantly increase awareness levels of glaucoma among target populations.
Though ‘family members and friends’ were not the main source of information about glaucoma in this study, being aware of a family history of glaucoma was strongly associated with glaucoma awareness (p<0.001). A positive family history is one of the risk factors of glaucoma, and this finding highlights the invaluable role of glaucoma patients as agents of awareness creation among their families and other contacts.
People who had had some formal education as opposed to no formal education were also more likely to be aware of glaucoma in this, as well as other studies.11 13 27
Awareness of the existence of a chronic, symptomless disease may be a key step towards control of that disease, but a good knowledge of the condition is pertinent for good compliance with the management plan. Knowledge about glaucoma in this study (36.8%) was better than findings in other settings.11 13 27 Higher glaucoma knowledge scores were observed among participants with higher educational attainment. This group of people may have better access to relevant information from the mass media (the most common source in this study) and other sources than their counterparts. The association between occupation and knowledge about glaucoma in this study may likely be due to the significant association between educational attainment and occupation also noted.
Furthermore, although awareness of family history and previous eye check were significantly associated with awareness in this study, this was not the case with knowledge. This underscores the importance of tailoring the content of awareness efforts to suit the needs of the intended audience. Good knowledge of glaucoma may enhance health-seeking behaviour among citizens and enable both patients and their family members cope with the demands of the life-long management of the condition.
The proportion of people with glaucoma in this study population (14.5%) was higher than that in other studies in Nigeria4 28 and its environs,29 though these were prevalence studies. Participants were also mostly of the Igbo ethnic group (99.2%), which had the highest prevalence of glaucoma from the Nigerian blindness and visual impairment survey.4 The greater prevalence with increasing age noted in other studies4 28 29 was also noted in this study, but there was no significant difference in terms of sex. About one in five people (19.1%) was blind with presenting vision <3/60 in the better eye, which is comparable with results of the national survey.4
The high number of glaucoma suspects (n=89/469, 19%) and cases (n=68/469, 14.5%) identified, as well as the number of cases blind thereof (n=13/68, 19.1%), makes a strong case for the usefulness of screening programmes in early detection of glaucoma in high-risk populations such as Nigeria until better screening strategies are developed.
One limitation of this study is that it was carried out on an outreach population that may undermine the generalisability of its results. Nevertheless, participants were from a varied mix of occupational, educational and demographic backgrounds, and some key findings were comparable with results of the national survey. The findings therefore provide important evidence for planning of public health measures for glaucoma control in terms of content, target population and medium.
References
Footnotes
Contributors All the authors have read and approved the final draft of the manuscript, and satisfied the conditions for authorship. All the authors agree that this work represents their honest contribution towards the writing of this manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.