Article Text

Statistics from Altmetric.com
Limited prospective data exist to inform management of eyes with centre-involved diabetic macular oedema (CI-DMO) and good visual acuity (VA). Results of the randomised, single-masked, three-arm Diabetic Retinopathy Clinical Research Network Protocol V trial led some to conclude a management strategy of clinical observation with initiation of intravitreal antivascular endothelial growth factor (anti-VEGF) on visual deterioration is appropriate.1 This interpretation is primarily based on the absence of a statistically significant difference in the primary outcome of vision loss at 2 years between eyes that received prompt aflibercept versus those assigned to observation and treated with aflibercept when VA worsened by 5–9 letters at two consecutive visits or ≥10 letters at one visit.1
The Protocol V findings, particularly the subsequent broad interpretation of observation as the preferred first-line management strategy, have kindled much debate.2 There is certainly a case for initial observation given the similar outcome for the proportion of patients with ≥5-letter loss at 2 years, which was 16% in the prompt aflibercept arm versus 19% in the observation arm. Furthermore, there was no significant difference between the prompt aflibercept and observation arms in the mean change from baseline VA (0.9 and −0.4 letters, respectively) or central subfield thickness (−48 and −42 µm, respectively) at 2 years.1 Retinal thickening can resolve spontaneously without treatment; indeed, in Protocol V, CI-DMO resolved without aflibercept treatment in 31% of eyes by 2 years in the observation arm.3 In addition, a first-line management strategy with observation can reduce the treatment burden, cost and inherent risk associated with intravitreal injections. However, this approach may not be appropriate for all patients with CI-DMO and good vision. Integral to achieving optimal efficacy with anti-VEGF treatment in general is the concept of delivering the right amount of treatment at the optimal time.4 To facilitate interpretation of the Protocol V outcomes and discuss the potential shortcomings of delaying treatment initiation in all cases, we present relevant evidence to consider from the VISTA and VIVID phase III trials which, in contrast with Protocol V, enrolled patients with more severe CI-DMO causing vision loss at baseline.5
First, the rates of ≥5-letter and ≥10-letter loss in a patient population with mild CI-DMO in the prompt aflibercept arm of Protocol V were substantially higher than in patients with worse CI-DMO in VISTA and VIVID who were treated with aflibercept 2 mg every 8 weeks after 5 initial monthly injections (2q8) (≥5-letter loss: 16% in Protocol V vs 4.6% and 10.4% in VISTA and VIVID, respectively; ≥10-letter loss: 9% vs 1.3% and 3.7%, respectively).1 5 The different rates of vision loss across these trials may simply reflect a floor effect limiting the potential for further vision deterioration in patients with worse CI-DMO and VA at baseline in VISTA and VIVID. However, 40.9% and 34.6% of patients in the laser arms of VISTA and VIVID, respectively, had worsening of DMO and lost an additional ≥10 letters at two consecutive visits or ≥15 letters at one visit through 2 years, and hence received rescue aflibercept 2q8 treatment as prespecified in the study protocol.5 These data suggest a substantial number of patients with severe CI-DMO and low VA can have further, clinically meaningful vision loss. Therefore, the higher rate of ≥5-letter and ≥10-letter loss may indeed indicate meaningful undertreatment in the prompt aflibercept arm of Protocol V compared with aflibercept 2q8 dosing in VISTA and VIVID over 2 years (8.3 vs 13.5 and 13.6 injections, respectively: ~39% lower dosing in Protocol V), but particularly in year 2 (2.4 vs 5.1 and 4.9 injections: ~52% lower dosing in Protocol V).1 5 An important consequence of undertreatment in the prompt aflibercept arm of Protocol V was setting a lower bar to compare efficacy with patients randomised to the observation arm who received delayed aflibercept treatment. In Protocol V, this theoretically led to smaller differences between the prompt aflibercept and initial observation arms than would have been seen with more consistent anti-VEGF therapy.
Second, a prespecified secondary endpoint of Protocol V was the proportion of eyes with VA of ≥84 letters (Snellen equivalent of ≥20/20). Despite undertreatment in the prompt aflibercept arm, a clinically meaningful larger proportion of eyes achieved a VA of 20/20 at 2 years compared with initial observation (77% vs 66%, respectively; 18% higher rate of achieving ≥20/20 vision with prompt aflibercept, p=0.03).1
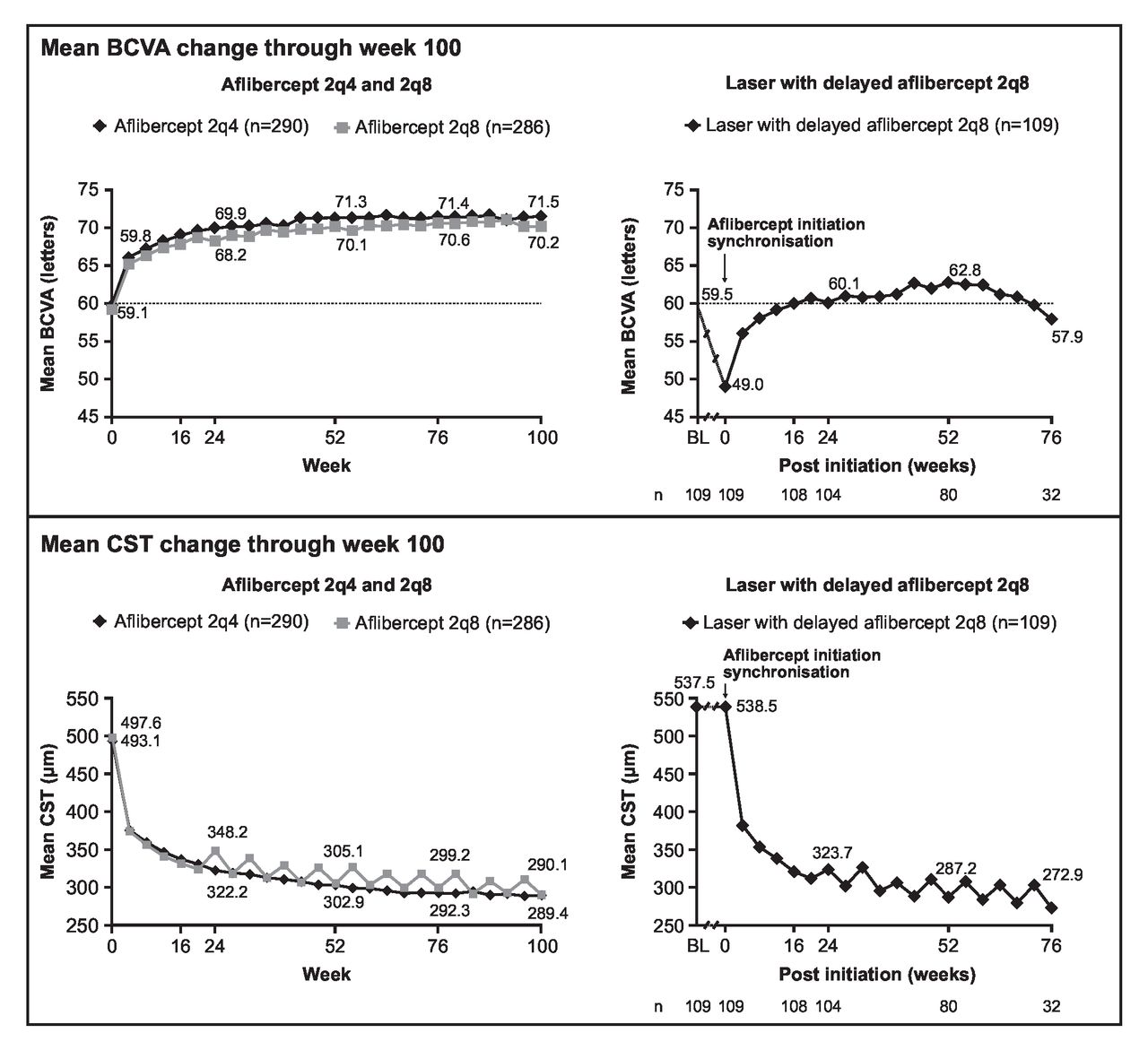
Third, several studies have provided opportunities to evaluate the consequence of delayed anti-VEGF treatment among patients with CI-DMO and VA loss. In VISTA and VIVID, eyes randomised to laser photocoagulation could receive aflibercept starting at week 24 if they lost ≥15 letters at one visit or ≥10 letters at two consecutive visits.5 At baseline, this subgroup of eyes (n=109) had a similar VA to those in the aflibercept 2q8 arm (59.5 vs 59.1 letters, respectively) (figure 1, upper panel).6 These eyes subsequently lost a mean of 10.5 letters to meet the protocol criteria to receive the same dosing regimen as prescribed to the 2q8 arm through week 100. After treatment with aflibercept following the initial delay, these eyes gained an average of 8.9 letters, nearly returning to their baseline VA (57.9 vs 59.5 letters, respectively) but not achieving the final absolute VA gains of those eyes initiated on aflibercept 2q8 from study start, with an ultimate clinically meaningful gap in visual outcomes of >12 letters (57.9 vs 70.2 letters, respectively) (figure 1, upper panel).6 In contrast, final absolute retinal thickness at week 100 was similar between eyes that received delayed aflibercept treatment and those that received aflibercept 2q8 from the start (272.9 vs 290.1 µm, respectively) (figure 1, lower panel). These findings indicate that while close-to-normal retinal thickness may be attainable, prolonged CI-DMO may inflict retinal damage that renders eyes incapable of achieving their maximal potential visual improvement when anti-VEGF treatment initiation is delayed. Similar findings were seen in the RIDE and RISE trials in which delayed anti-VEGF therapy with ranibizumab resulted in lower VA gains and lower absolute VA levels compared with prompt anti-VEGF therapy initiation.7

{kind=link}
Visual and anatomic outcomes following early and delayed aflibercept for CI-DMO from pooled analysis of VISTA and VIVID.6 Eyes received aflibercept 2q4 and 2q8, or laser with delayed aflibercept 2q8 following further vision loss. Mean change in BCVA (upper panel) and CST (lower panel) through week 100 are shown. Mean BCVA and mean CST with laser with delayed aflibercept 2q8 were synchronised at the time of aflibercept initiation. The analyses included data after rescue. From week 12, study eyes in the laser control group were assessed and received macular laser photocoagulation up to every 12 weeks if ETDRS-defined clinically significant DMO was present (defined as thickening of the retina or hard exudates at ≤500 μm of the centre of the macula or at least one zone of retinal thickening one disc area or larger, any part of which was within one disc diameter of the macula centre).5 Study eyes in the laser control group could also receive aflibercept treatment from week 24 onwards if DMO worsened causing either a ≥15-letter VA loss from the best previous measurement at one visit or a ≥10-letter VA loss from the best previous measurement at two consecutive visits, with no improvement in BCVA from baseline. Eyes meeting these criteria received five monthly injections of aflibercept, followed by aflibercept 2q8, and continued to receive active macular laser photocoagulation per laser retreatment criteria. Eyes could receive both laser and intravitreal aflibercept injection, when applicable, at the same visit.5 2q4, 2 mg every 4 weeks; 2q8, 2 mg every 8 weeks; BCVA, best-corrected visual acuity; BL, baseline; CI-DMO, centre-involved diabetic macular oedema; CST, central subfield thickness; ETDRS, Early Treatment Diabetic Retinopathy Study; VA, visual acuity.
This phenomenon of delayed treatment leading to suboptimal final visual outcomes may also be found in the Protocol V data. The subset of eyes that was randomised to initial observation and subsequently received aflibercept (37%) had an average VA of 84.8 letters (median Snellen equivalent 20/20) at baseline and completed the study with a loss of nearly five letters, or an average VA of 80.0 letters (median Snellen equivalent 20/25).3 This decline suggests that delaying anti-VEGF treatment initiation may have resulted in suboptimal final visual outcomes in eyes with CI-DMO and good vision and, more concerningly, vision loss that cannot be regained with undertreatment.
The mandated and protocol-defined close monitoring of patients enrolled in clinical trials can be quite distinct from practice patterns in routine clinical practice; real-world patients are more likely to exhibit lower visit adherence and have poor systemic disease control,8 9 both of which are intentionally minimised in clinical trial settings. Therefore, lower adherence to monitoring visits in routine clinical practice is likely to result in more substantial vision loss over time. Undertreatment of such patients may potentially lead to worse visual outcomes compared with patients in Protocol V who had better systemic disease control and consistent monitoring, enabling more timely intervention once vision or anatomy worsened.
The totality of evidence suggests that the frequency and timing of anti-VEGF treatment are important factors to consider for achieving optimal outcomes through early normalisation of retina anatomy in patients with CI-DMO, regardless of baseline VA. These factors must be carefully considered along with associated disease characteristics such as diabetic retinopathy severity, fellow eye status3 and ability to adhere to clinical appointments when designing individualised management strategies that maximise patient benefit.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Medical writing support was provided by Linda Brown, BSc (Hons), of Core (Oxford, UK) according to Good Publication Practice guidelines (http://annals.org/aim/article/2424869/good-publication-practice-communicating-company-sponsored-medical-research-gpp3).
Footnotes
Contributors All authors contributed to interpretation of the data, critically revising the manuscript content, and all authors approved the final version.
Funding This study was funded by Regeneron Pharmaceuticals, Inc.
Competing interests DVD reports serving as a consultant for Allergan, Asclepix, Boehringer Ingelheim, Clearside, Genentech, Kodiak Sciences and Regeneron Pharmaceuticals, Inc.; and receiving research funding from Asclepix, Boehringer Ingelheim, Genentech and Regeneron Pharmaceuticals, Inc. HM is an employee and shareholder of Regeneron Pharmaceuticals, Inc. CCW reports serving as a consultant for Acucela, Adverum, Aerpio, Alcon, Alimera Sciences, Allergan, Alnylam, Apellis, Arctic Vision, Bausch + Lomb, Bayer, Bionic Vision Technologies, Chengdu Kanghong Biotechnologies, Clearside Biomedical, Corcept Therapeutics, DORC, EyePoint, Genentech, Gyroscope, IVERIC Bio, Kodiak Sciences, Merck, NGM Biopharmaceuticals, Notal Vision, Novartis, OccuRx, ONL Therapeutics, Opthea, Oxurion, Palatin, Polyphotonix, Recens Medical, Regeneron Pharmaceuticals, Inc., RegenXBio, Roche, Santen, Takeda, Thea Open Innovation and Verana Health; receiving grants for research support from Adverum, Aerie Pharmaceuticals, Aldeyra, Allergan, Apellis, Boehringer Ingelheim, Chengdu Kanghong Biotechnologies, Clearside Biomedical, Gemini Therapeutics, Genentech, Graybug Vision, Gyroscope, IONIS Pharmaceutical, IVERIC Bio, Kodiak Sciences, LMRI, Mylan, Neurotech Pharmaceuticals, NGM Biopharmaceuticals, Novartis, Opthea, Outlook Therapeutics, Recens Medical, Regeneron Pharmaceuticals, Inc., RegenXBio, Roche, Samsung Bioepis, Santen, Senju, Taiwan Liposome Company, and Xbrane BioPharma; and receiving speaker fees for speaker’s bureau from Regeneron Pharmaceuticals, Inc.
Provenance and peer review Not commissioned; externally peer reviewed.