Article Text

Abstract
Objective To assess the long-term efficacy and safety of accelerated transepithelial corneal cross-linking (ATE-CXL) with 30 mW/cm2 × 3 min.
Methods and Analysis Thirty-four eyes of 23 patients with progressive keratoconus (KCN) recruited within a single centre were enrolled in this prospective interventional study. Exclusion criteria included: history of Descemet’s membrane rupture, glaucoma, uveitis, severe dry eye, concurrent corneal infections, and systemic disease that could affect corneal healing. ATE-CXL was performed with 3 min of ultraviolet-A continuous irradiation (30 mW/cm2). Follow-up examinations were scheduled on postoperative day 1; 1 and 2 weeks; 1, 3 and 6 months; and 1, 2 and 3 years. Main outcome measures were maximum corneal power (Kmax), average corneal power (AvgK), steepest corneal power (Ks), central corneal thickness, thinnest corneal thickness, uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity (BCVA) and endothelial cell density.
Results Mean Kmax, AvgK, Ks, UCVA, BCVA and endothelial cell density did not significantly change over 3 years. The speed of progression obtained by linear regression analysis on corneal parameters (Kmax, AvgK, Ks) improved after ATE-CXL. All baseline parameters correlated with the postoperative Kmax slope. Two eyes underwent ATE-CXL redo because of continued progression after the primary CXL.
Conclusion This is the first report of 3-year results of ATE-CXL with 30 mW/cm2 × 3 min. ATE-CXL (30 mW/cm2 × 3 min) was safe and effective for slowing down KCN progression.
Trial registration number This study was registered with ID UMIN000009372 in UMIN-Clinical Trials Registry.
- cornea
- degeneration
- treatment surgery
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Accelerated transepithelial cross-linking (ATE-CXL) with 30 mW/cm2 ultraviolet A irradiation for 3 min is a minimally invasive method and it takes the shortest-procedure time of the practical methods. However, long-term results of this method over 2 years have not reported.
What are the new findings?
ATE-CXL with 30 mW/cm2 × 3 min was safe and effective for slowing down keratoconus progression after 3 years follow-up.
How might these results change the focus of research or clinical practice?
ATE-CXL with 30 mW/cm2 × 3 min is worth considering for some cases in which removal of the epithelium is difficult, such as in advanced cases with a thin cornea.
Introduction
Corneal cross-linking (CXL) was recently recognised as a preventive treatment for keratoconus (KCN).1 CXL increases the biomechanical stiffness of the cornea by inducing a photochemical reaction between riboflavin, a photosensitiser and ultraviolet A (UVA), which can be enhanced by supplementary oxygen2 3 The standard Dresden protocol, which included central corneal epithelium removal and 0.1% riboflavin instillation into the cornea for 30 min before UVA irradiation, was first reported in 2003.4 In this protocol, a 3 mW/cm² UVA irradiation intensity is applied for 30 min. With long-term observation of over 10 years, previous studies have demonstrated the effectiveness of the standard protocol to halt KCN progression.5–7 This protocol, however, has two major disadvantages: the risk for complications associated with epithelial removal, such as postoperative corneal opacity and keratitis,8 and a long procedure time of approximately an hour. To ameliorate the disadvantages of the standard protocol, many attempts have been made to modify the CXL protocol. Transepithelial CXL along with implantation of Intacs (Corneagen, Seattle, Washington, USA) for patients with KCN was first reported in 2009. In this procedure (Epi-on), epithelial removal is avoided by using a 0.1% riboflavin-5-phosphate solution with 20% dextran,9 followed by the administration of topical drugs such as EDTA, benzalkonium chloride, gentamicin and/or trometamol to enhance the epithelial permeability.10 11 Riboflavin iontophoresis is another approach for the Epi-on CXL.12–14 CXL of riboflavin without epithelial removal reduces the risk of complications, such as postoperative infection, and persistent epithelial defects and opacities.15 Actually microbial keratitis is not uncommon after epithelium-off (Epi-off) CXL, especially when performed, followed by bandage contact lenses or topical steroids.16 Another approach is accelerated CXL, which was first reported in 2012.17 This modification is based on the Bunsen-Roscoe law,18 according to which the rate of the photochemical and photobiological reaction is directly proportional to the total dose of radiation energy (eg, 30 mW/cm² UVA for 3 min,17 18 mW/cm² UVA for 10 min,19 9 mW/cm² UVA for 10 min19). By applying higher UVA intensities, accelerated CXL reduces the duration of the procedure. According to meta-analyses, the standard protocol is more favourable for halting the progression of KCN than transepithelial CXL11 and accelerated CXL20 21 with relatively mild irradiation intensities (eg, 9 mW/cm² for 10 min, 18 mW/cm² for 5 min), whereas high irradiation intensity for a short period of time (30 mW/cm² for 3 min) induces corneal flattening equal to that achieved by the standard protocol.20 Transepithelial CXL is less effective but provides better visual outcomes compared with the standard protocol.11
Accelerated transepithelial CXL (ATE-CXL) is a newly introduced method that takes advantage of both methods; it is not only less invasive but also takes less time. The efficacy of ATE-CXL has reported since 2016 and the longest follow-up periods reported are 4 years in adults22 and 3 years in children.23 However, most of those studies were performed with the UV-A irradiation setting of 45 mW/cm2 × 5 min 20 s, pulse, and there has not been reported the long-term clinical results of ATE-CXL of 30 mW/cm2 × 3 min, continuous. To assess the efficacy and safety of ATE-CXL, we conducted a prospective study of ATE-CXL from 2012 to 2018. Here, we report our 3-year clinical results of ATE-CXL (30 mW/cm2 × 3 min).
Methods
Patients
We consecutively enrolled patients recruited from among outpatients at the Department of Ophthalmology, the University of Tokyo Hospital, between October 2012 and October 2018.
Patient and public involvement
We provided basic information about treatment by a face-to-face consultation to help in better understanding of research concepts, research question, choice of other treatment or protocol. As results were obtained, we reviewed the results with patients in personal consultations to help their informed consents and better effective and satisfying choices.
Inclusion and exclusion criteria
Inclusion criteria were age over 14 years, clinical diagnosis of KCN, and clinical evidence of progression with the thinnest corneal thickness (TCT) measuring >380 µm before UVA irradiation, as recommend by the transepithelial CXL protocol. KCN progression was primarily determined by an increase in the maximum corneal power (Kmax) greater than 1 dioptre (D) in the central area with a 10 mm diameter, and secondarily assessed by an increase in the mean spherical refractive equivalent to 1D, and an increase in astigmatism of 1D in 2 years. Patients were excluded from the study if they had a history of Descemet’s membrane rupture; glaucoma; uveitis; severe dry eye; concurrent corneal infections; or systemic disease that could affect corneal healing, such as diabetes mellitus. In addition, pregnant or lactating women were excluded from the study.
Surgical procedure and measurement
All patients underwent ATE-CXL (KXL, Avedro, Massachusetts, USA). After applying topical anaesthesia (4% lidocaine and 0.4% oxybuprocaine hydrochloride), the corneal surface was treated with 0.25% riboflavin solution supplemented with benzalkonium chloride, EDTA, trometamol, hydroxypropyl-methylcellulose (ParaCell Part1, Avedro) for 4 min, and then 0.25% riboflavin solution (ParaCell Part 2, Avedro) for 6 min. During the soak time, an additional drop was applied before finishing. The central corneal thickness (CCT) was measured with a handheld ultrasound pachymeter (Handy Pachymeter, SP-100, TOMEY, Japan). If the CCT was thinner than 380 µm, distilled water was applied until the thickness condition was satisfied. UVA treatment at a 370 nm wavelength was continuously performed at an irradiance of 30 mW/cm2 for 3 min, delivering a dose of 5.4 J/cm2 without corneal epithelial debridement. After irradiation, optical antibiotic ointment (0.3% ofloxacin) was instilled and an eye bandage was applied for 1 day. An antibiotic and corticosteroid (1.5% levofloxacin, 0.1% fluorometholone) were topically applied.
Before recruitment for this study, all patients were followed up more over three times. Patients were instructed to visit the clinic before surgery as baseline and at 1 and 2 weeks; 1, 3 and 6 months; and 1, 2, and 3 years postoperatively as fixed-point observation days. Preoperative and postoperative examinations included uncorrected visual acuity (UCVA), best spectacle corrected visual acuity (BCVA), Kmax in the central area of 10 mm in diameter, average corneal power (AvgK), steepest corneal power (Ks), CCT, TCT evaluated by anterior segment optical coherence tomography (CASIA SS-1000, SS-2000, TOMEY, Japan), endothelial cell density (ECD) evaluated by specular microscopy (FA-3809, KONAN Medical, Japan), intraocular pressure evaluated by applanation tonometry, and non-mydriatic indirect fundus examination. Patients were also asked to report any pain or discomfort during the procedure at each visit.
We also analysed the speed of change in these parameters. Parameter changes over time (slope) during the preoperative period and those occurring from postoperative 1 month to 3 years were analysed by linear regression in eyes that received anterior segment optical coherence tomography more than three times preoperatively and for more than 3 years postoperatively. All measured data other than at the time of the prescribed visit were also included for calculating the slope.
Statistical analysis
The Steel-Dwass test was used to evaluate changes in the postoperative parameters at each visit vs the preoperative measurements. The Wilcoxon signed-rank test was used to compare preoperative and postoperative slopes. Correlations between preoperative mean parameters and postoperative slopes were evaluated by the restricted maximum likelihood method. A p<0.05 was considered significant. Statistical analyses were performed using JMP-11 software (SAS Institute). Missing data were handled by listwise deletion.
Results
A total of 90 eyes underwent primary ATE-CXL for progressive KCN and 34 eyes (30 eyes of males (88%), 4 eyes of females (12%)) of 23 patients (21 males, 2 females) that were followed up for postoperative 3 years were included in this study. Mean patient age was 26.8±8.0 (range 16–44) years. All surgeries performed on 34 eyes were uneventful, without intraoperative complications. All of 34 eyes underwent preoperative and postoperative 1 weeks and 3 years examination. The number of missing data at 2 weeks, 1, 3 and 6 months; and 1 and 2 years postoperatively were 5, 5, 4, 3, 2 and 1, respectively. Data missing was caused by deviation of date of visit.
After ATE-CXL, mean UCVA, BCVA, ECD, Kmax, AvgK, Ks, CCT and TCT showed no statistically significant change over time up to 3 years (figure 1). (Detailed results are shown as online supplemental material.) The rate of an increase in Kmax of 1D or more in each participant at 1, 2 and 3 years compared with baseline was 18%, 19% and 30%, respectively.
Supplemental material
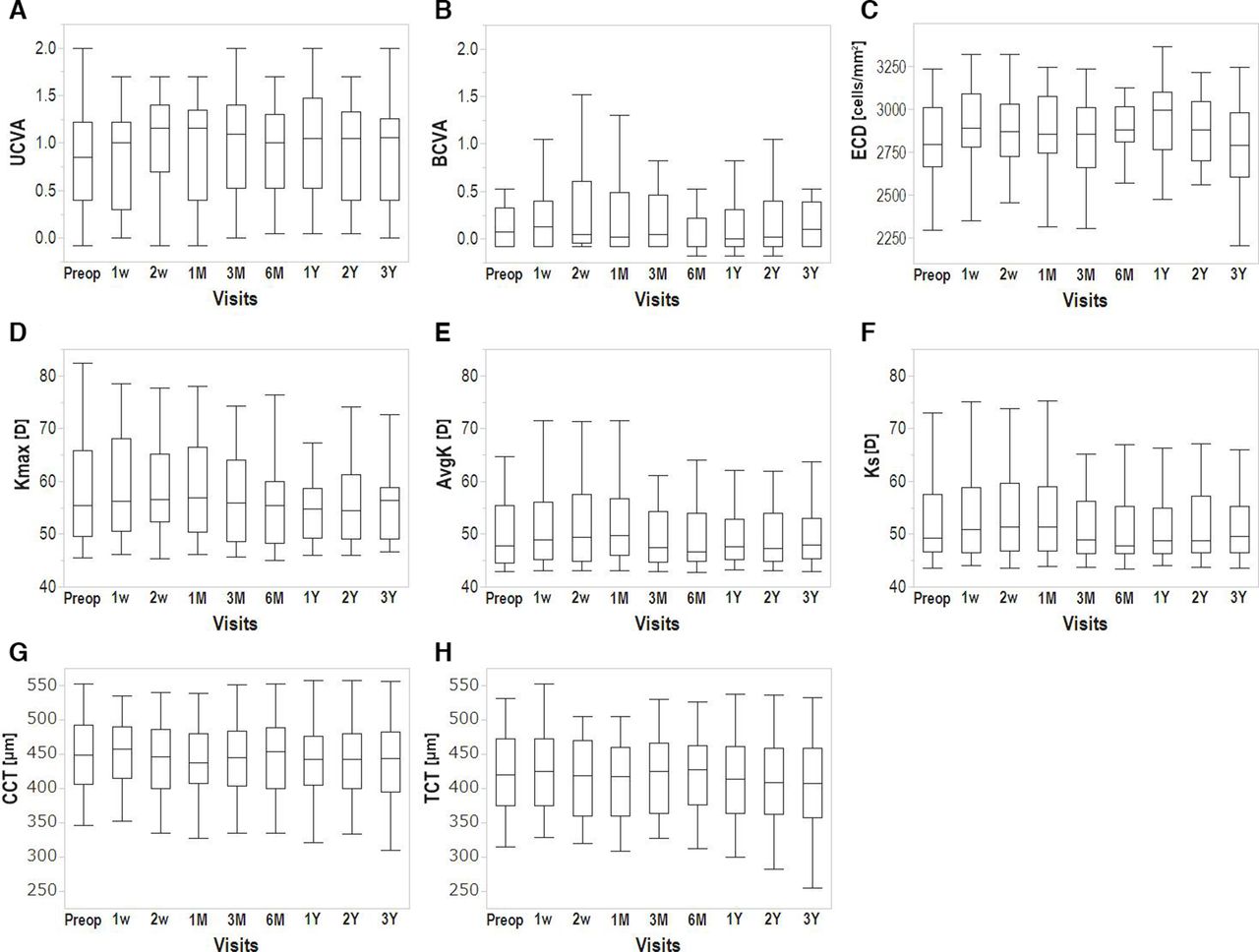
Changes from baseline to postoperative 3 years after ATE-CXL. (A) Uncorrected visual acuity (UCVA), (B) best spectacle-corrected visual acuity (BCVA), (C) endothelial cell density (ECD), (D) maximum corneal power (Kmax), (E) average corneal power (AvgK), (F) steepest corneal power (Ks), (G) central corneal thickness (CCT), (H) thinnest corneal thickness (TCT). UCVA, BCVA, ECD, Kmax, AvgK, Ks, TCT and CCT showed no significant change over time for up to 3 years (Steel test). ATE-CXL, accelerated transepithelial corneal cross-linking; D, dioptre.
The mean Kmax, AvgK, Ks slopes improved significantly after ATE-CXL. The mean CCT slopes also improved but the mean TCT slopes worsened slightly (table 1). The number of cases in which the postoperative slope was smaller than the preoperative slope was as follows: Kmax, 27 eyes (79%); AvgK, 26 eyes (76%); Ks, 28 eyes (82%); CCT, 26 eyes (76%) and TCT, 24 eyes (70%). Figure 2 shows the distribution of the postoperative Kmax slopes calculated by linear regression. In 30 (88%) of 34 eyes, the Kmax slope was less than +1D per year after ATE-CXL.

{kind=link}
{kind=link}
Distribution of Kmax slopes after ATE-CXL. The slope was obtained by linear regression to approximate the progression speed at 3 years after ATE-CXL. ATE-CXL, accelerated transepithelial corneal cross-linking; D, dioptre; Kmax, maximum corneal power.
Preoperative versus postoperative slope comparison
The mean baseline parameters (Kmax, AvgK, Ks, CCT and TCT) weakly correlated with the postoperative Kmax slope (table 2). The baseline Kmax, AvgK, Ks and postoperative Kmax, AvgK, Ks slope were negatively correlated. Baseline CCT and TCT were positively correlated with a postoperative Kmax slope.
Correlation coefficients between baseline mean parameters and postoperative slopes
Complications
Most patients experienced dull pain for 1 or 2 days postoperatively, but improved soon thereafter. Two eyes (5.9%) of 2 male patients worsened after primary ATE-CXL and underwent an ATE-CXL redo.
Discussion
In this study, we first report the 3 year results of ATE-CXL (30 mW/cm2 × 3 min) to evaluate the safety and efficacy of the procedure for preventing KCN progression. Neither BCVA, UCVA, nor ECD changed during the observational period after ATE-CXL. Those findings confirm the safety of ATE-CXL and are consistent with the safety established in meta-analyses of the other CXL protocols, for example, standard, Epi-on or accelerated.11 20 21
Keratometric parameters, such as Kmax, AvgK and Ks, and corneal thickness remained stable for 3 years. Considering the progressive nature of KCN, the finding that these parameters did not change indicates that ATE-CXL effectively suppressed the KCN progression to some extent. Many reports regarding the standard protocol, however, showed a decrease in the mean Kmax and other keratometric parameters over time.24–27 In terms of corneal flattening, ATE-CXL might not be as sufficient, similarly to the Epi-on or accelerated protocols.11 20 21 28
Table 3 shows the results of previous reports about ATE-CXL for KCN. Our study with the setting of 30 mW/cm2 × 3 min compares favourably with previous ATE-CXL studies with the setting of 45 mW/cm2 × 5 min 20 s, pulse; Averages of keratometric parameters and visual acuities were stable during follow-up periods.
The current study and past reports of ATE-CXL for keratoconus
Judging KCN progression only on the basis of keratometric values at each time-point is problematic, however, in that they are often erroneous, especially in irregularly shaped corneas like those with KCN; a measurement variance of ~1D is quite common. Thus, we used a linear regression model to remove the erroneous measurement values. This method was introduced in the previous report to judge the transitional changes of corneal shape in KCN eyes,29 and also similar analyses (called Trend analysis) are available in CASIA. Calculating the slopes by linear regression allowed us to visualise the ‘speed’ of the progression.
The postoperative slopes were generally favourable compared with the preoperative slopes. Mean slopes of Kmax, AvgK and Ks turned negative postoperatively, indicating improvement. Mean CCT slopes were also improved but increment of mean TCT slopes indicated persistent corneal thinning at the lesion area. Overall, KCN progression was halted in most of the patients with approximately 0 D/y and ~88% of the eyes were stable 3 years after ATE-CXL.
In the correlation analyses, all baseline parameters correlated with postoperative Kmax, but most did not correlate with the slopes of the other postoperative measures. Only baseline TCT values correlated with three keratometric parameters (Kmax, AvgK and Ks). This suggests that CXL is more effective for a thinner cornea. This may be because the proportion of stromal volume that is cross-linked should increase more in a thinner cornea, if the demarcation line depth of 150–200 μm30 is constant.
Two cases required CXL redo because of postoperative KCN progression. These 2 cases received the redo over 3 years after primary CXL. One case showed continuous worsening in Kmax, and another was stable for 3 years but rapid Kmax progression was seen after 3 years. Actually, the redo rate of our study (5.9%) seems higher than previous reports of Antoun et al,31 who reported a 3% redo rate for the standard protocol. This may be a limit of ATE-CXL efficacy, although ATE-CXL redo rates have not been reported to date. Tzamalis et al recently reported a review on repeated CXL.32 The possible inefficacy of Epi-on CXL compared with Epi-off CXL is implied by a meta-analysis11 or by a redo case series of Akkaya Turhan et al,33 in which, among 12 eyes of CXL re-do cases, 9 eyes were of primary Epi-on CXL while 3 eyes were of primary Epi-off CXL.
As described above, ATE-CXL was effective in most cases in our prospective study, although some patients developed KCN progression even after ATE-CXL. It is true that even after using a linear regression model, 12% of patients showed progression. Although there are no reports which evaluate post-CXL KCN progression using linear regression model and cannot simply compare the present results to the past, the result may be a limit of ATE-CXL efficacy. Thus, we suggest that ATE-CXL is not for all patients who has progressive KCN but for some patients who can possibly enjoy the benefit of not removing epithelium, for example, patients who do not have enough corneal thickness for Epi-off CXL or who are vulnerable to infection having severe atopic dermatitis etc. Actually, ATE-CXL procedure can be safely performed in less time than the standard procedure, and can be performed in more advanced cases with <420 µm TCT, which is not suitable for Epi-off procedure. Finding optimal cases for ATE-CXL in terms of safety and efficacy is a subject of future investigation.
A limitation of this study is the limited number of patients. Further follow-up of more patients is needed. Another limitation is that we did not assess the posterior keratometric change, whose importance34 is emphasised in the global consensus35 which was published after our study had started.
Conclusion
This is the first report of 3-year results of ATE-CXL with 30 mW/cm2 × 3 min. ATE-CXL with 30 mW/cm2 × 3 min is safe and effective for slowing down KCN progression even in a long-term follow-up. Even with reference to the previously reported results of ATE-CXL with 45 mW/cm2 × 5 min 20 s, pulse, the results of ATE-CXL with 30 mW/cm2 × 3 min were equally effective in halting the deterioration of visual acuities and keratometric and pachymetric parameters. ATE-CXL is worth considering for some cases in which removal of the epithelium is difficult, such as in advanced cases with a thin cornea.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study adhered to the tenets of the Declaration of Helsinki. All patients received an explanation of the study protocol and provided written informed consent to participate in the study. The Institutional Review Board/Ethics Committee of the University of Tokyo approved the study (approval number P2011034-11Y).
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
HI and JY contributed equally.
Contributors HI and JY contributed equally to this study. The authors who contributed to the design and conduct of the study were HI, JY and TM; to the collection, management, analysis, and interpretation of data were HI and JY; and to the preparation, review and approval of the manuscript was HI, JY, TT, SY, TU and TM. JY acts as guarantor for the study.
Funding This work was supported by JSPS KAKENHI (grant number JP18K16917 and JP18K16947).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.