Article Text

Abstract
Objective Increasingly, cornea banks are recovering donor tissue from pseudophakic donors. Little is known about their suitability for Descemet membrane endothelial keratoplasty (DMEK) surgery in terms of endothelial cell density (ECD) and preparation failure.
Methods and Analysis We explored ECD during donor tissue preparation in 2076 grafts. Preparation failure was analysed in 1028 grafts used in DMEK surgery at our clinic. To monitor ECD and functional results, we matched 86 DMEK patients who received pseudophakic donor grafts with similar recipients of phakic donor grafts and followed them up for 36 months.
Results At recovery, mean ECD in pseudophakic donor grafts was 2193 cells/mm2 (SD 28.7) and 2364 cells/mm2 (SD 15.7) in phakic donor grafts (p<0.001). After cultivation, the difference increased as pseudophakic donor grafts lost 14% of ECD while phakic lost only 6% (p<0.001). At transplantation, mean ECD in pseudophakic donor grafts was 2272 cells/mm2 (SD 250) and 2370 cells/mm2 (SD 204) in phakic donor grafts (p<0.001). After transplantation, the difference in ECD increased as pseudophakic donor grafts lost 27.7% of ECD while phakic donor grafts lost only 13.3% (p<0.001). The risk of preparation failure in pseudophakic donor grafts was higher than in phakic donor grafts (OR 4.75, 95% CI 1.78 to 12.67, p=0.02). Visual acuity increased in both groups similarly.
Conclusions Pseudophakic donor grafts have a lower ECD, are more prone to endothelial cell loss during recovery and surgery and are associated with a higher risk of preparation failure. Cornea banks and surgeons should consider this in the planning of graft preparation and transplantation.
- cornea
- dystrophy
- treatment surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Graft tissue from pseudophakic donors tends to have a lower endothelial cell density.
What are the new findings?
Graft tissue from pseudophakic donors is more susceptible to endothelial cell loss during the cultivation process and during surgery. Preparation failure of donor lamella is more frequent in pseudophakic donor grafts. This can lead to a higher rate of pseudophakic donor grafts that are lost or not suitable for elective transplantation.
How might these results change the focus of research or clinical practice?
Cornea banks and surgeons should consider the differences between phakic and pseudophakic donor grafts during cultivation and surgery.
Introduction
Descemet membrane endothelial keratoplasty (DMEK) has become a standard technique to treat corneal endothelial dystrophies. Different from other posterior lamellar keratoplasty techniques, such as Descemet stripping automated endothelial keratoplasty (DSAEK), DMEK surgery comprises a transplantation of endothelium and Descemet membrane (DM) only.1 The procedure is challenging, including the donor tissue preparation, but has proven to be superior in terms of visual recovery and immunological reactions, when compared with DSAEK.2 3 As such, DMEK has already replaced DSAEK as the standard procedure in some parts of Europe and the USA.4 5
For a successful surgery, donor tissue quality is of importance. Donor tissue with high endothelial cell density (ECD), a donor age of above 60 years and the absence of corneal scars is preferred to assure long-term visual recovery, and facilitate donor DM preparation.6 7 Many surgeons prefer corneas from phakic donors, which mitigate difficulties during preparation as a result of corneal scars or adhesions following cataract surgery. In addition, tissue from older donors is preferable as unfolding such tissue is often easier than in younger donors.8–10 The ideal tissue, hence, has a high ECD and comes from an older phakic donor.8
Recovering donor tissue form older, phakic patients is becoming increasingly difficult. A survey conducted in the US population in 2004 showed a combined cataract prevalence in the age group over 40 years of 17% with rates as high as 50% in the age group above 75 years.11 With increased life expectancy, cataract prevalence is expected to rise by 50% in the year 2020 and cataract surgery rates are expected to rise by over 60%.11 In fact, it has been shown that incidence of cataract surgery has been increasing over the past three decades and is unlikely to decline in the near future.12 Given these trends, cornea banks will increasingly recover corneas of pseudophakic donors and provide them for transplantation.
Even though some DMEK surgeons are already using pseudophakic donor tissues,13 little is known about the differences between phakic and pseudophakic donor tissue. Some reports on DMEK surgeries using pseudophakic donor tissues suggest that ECD is lower than in phakic donors but that intraoperative and postoperative results are comparable.13 To explore how this difference could affect donor tissue preparation and postsurgical outcomes, we conducted a retrospective analysis of corneal transplants from the moment of recovery to 3 years after transplantation.
Methods
We conducted a retrospective analysis that explored donor graft tissues used in DMEK surgeries at our clinic between 2015 and 2018.
Collection of donor graft data
Collecting donor tissue was conducted by the cornea bank of the Charité-Universitätsmedizin Berlin. We reviewed donor records of all corneas donated between 2015 and 2018. Only records that recorded ECD at the beginning and after cultivation were included in the analysis.
Recovery of donor graft tissue and cultivation
All donor corneas were obtained by in situ corneoscleral disc excision. They were kept in organ culture (Minimum Essential Medium with 2% fetal calf serum) at 32°C±1°C. The ECD was estimated at the start of organ culture and 24±6 hours after transfer to dextran-containing deswelling medium prior release for transplantation, using at least two digital 200× images from an inverse phase contrast microscope (Olympus CK 40, Olympus, Hamburg, Germany) postosmotic stimulation with hypotonic balanced salt solution. The ECD was estimated using a fixed frame of maximum possible size with manual marking of the cells with the NAVIS cell counting software (Nidek Technologies, Padova, Italy). All measurements of ECD were done at the centre of the cornea. Morphological parameters (polymegatism, pleomorphism, vacuolisation and granulation) were assessed visually during endothelial cell microscopy and graded as no changes, mild changes or severe changes. Only corneas with no or mild changes were released for transplantation and included in this study.
Collection of recipient data
From the transplantation records we identified all grafts that were used at our clinic for DMEK surgery. The recipient case files were reviewed to identify DMEK patients without ocular comorbidities that could complicate the surgery or would lead to a reduced prognosis. We included phakic and pseudophakic patients with Fuchs endothelial dystrophy (FED), bullous keratopathy or first graft failure without a history of ocular surgeries (except cataract surgery). We also excluded all patients with a history of uveitis and uncontrolled glaucoma and patients who did not attend follow-up visits at our clinic. Based on these criteria, we identified suitable recipients of pseudophakic donor graft tissue and matched them to recipients of phakic donor graft tissue. We used possible confounders with an effect on ECD as matching criteria and matched on type of surgery, use of antiglaucoma eye-drops, history of diabetes and age (with a range of 5 years).
Surgical procedure and follow-up
All patients underwent DMEK surgery at out clinic with the same experienced surgeon (NT). In brief, after removal of the host’s DM, the graft was injected into the anterior chamber. After unfolding of the graft, the anterior chamber was filled with air aiming at a physiological or slightly elevated pressure. No iridotomy or iridectomy was performed. We partially removed the air 2 hours after the surgery. The donor tissue DM was prepared by the same surgeon directly prior to transplantation. The DM was dissected with a scraping technique from the periphery, gently teared with blunt forceps and punched centrally with a trephine of desired size (approximately 8.5 mm diameter). Standard postoperative topical treatment included steroids, antibiotics and lubricant eye-drops. Patients were followed up for 3 years. At each examination we tested best corrected visual acuity (BCVA) with a Snellen chart, performed a slit lamp examination and an optical coherence tomography (OCT) examination of the cornea using a Spectralis OCT device with an anterior chamber attachment (Spectralis OCT, Heidelberg Engineering Family Acquisition Module 5.3.3.0, Heidelberg Engineering Viewing Module 5.3.2.0 and Heidelberg Eye Explorer 1.6.4.0 software, Heidelberg Engineering, Heidelberg, Germany). The Snellen decimal number was converted in logMAR visual acuity using a conversion table. ECD was measured at the centre of the cornea using the specular microscope Nidek CEM-530 (NIDEK, Japan).
Statistical analysis
All data were entered into a database and checked for errors. We used STATA V.12.1 (StataCorp, College Station, Texas, USA) for statistical analysis and graphs were drawn using the ggplot2 module in R-statistics. Bivariable associations were tested using a χ2 or t-test, where appropriate.
For binary outcomes, we used a logistic regression model controlling for confounders. To model ECD over time, we used a mixed effects regression model controlling for repeated observations per individual and follow-up period as well as confounders. To explore the difference in the rate of endothelial cell loss (ECL), we measured the difference in the rate of ECL between pseudophakic and phakic donor tissues, controlling for confounders. With this approach, a difference of 0 would indicate that there is no difference in the rate of ECL between the two groups. This approach allows to explore the effect of donor lens status on ECD while controlling for baseline differences (such as donor age) between the two groups. We assumed a significance level of 0.05 and used a Bonferroni correction to account for multiple testing.
For the statistical analysis of BCVA, we excluded all patients with extracorneal limitations such as age-related macular degeneration or amblyopia.
Patient and public involvement
There was no patient involvement in planning and executing this study. We are planning to inform future patients when planning DMEK surgeries and the public via presentation of our findings on congresses and through publication.
Results
Pretransplantation
Between January 2015 and January 2018, we reviewed protocols of 3077 donor corneas. As ECD estimation at the beginning of organ culture is not always possible, we identified 2076 donor cornea protocols with complete ECD data. Of these, 392 (18.9%) were from pseudophakic donors.
Pseudophakic donors were older than phakic donors and there were a higher number of female donors (table 1). At recovery, pseudophakic donor grafts showed a lower ECD than phakic donor grafts (table 1). In both groups, ECD decreased after cultivation but ECL was higher in the pseudophakic group (table 1). In the pseudophakic group ECL was 14% while in the phakic group ECL was only 6%. Controlling for donor age and cultivation time, the rate of ECL was 105 cells (95% CI 56 to 153, p<0.001) higher in pseudophakic donor grafts than in the phakic donor grafts. This resulted in an increase in the mean difference in ECD between pseudophakic and phakic donor grafts (table 1). The lower ECD at recovery and the higher rate of ECL during cultivation meant that 196 (50%) of the pseudophakic donor corneas did not meet the minimum quality criteria for an elective graft (>2000 cells/mm2). In the phakic donor group, only 218 (13%) did not reach a minimum of 2000 cells/mm2 (p<0.001).
Characteristics of 2076 donors tissues
Post-transplantation
Of all recovered donor grafts, 1028 were used at our clinic for DMEK surgery. The remaining ones were either of too low ECD for an elective procedure, sent to other clinics for grafting or they were used in penetrating keratoplasty. The 1028 grafts included 126 pseudophakic donor grafts. Seven pseudophakic donor grafts were lost during preparation, and of the remaining 119 pseudophakic donor grafts, 33 had to be excluded as either the recipient did not meet with our inclusion criteria or they did not complete follow-up visits at our clinic.
Donor preparation
Preparation of donor grafts failed in 7 (5.6%) of the 126 pseudophakic donor grafts and in 17 (1.9%) of the 902 phakic donor grafts (p=0.011). Controlling for the donor age and cultivation time, we found that the risk of preparation failure was almost five times higher (OR 4.75, 95% CI 1.78 to 12.67, p=0.02) in pseudophakic donor grafts than in phakic donor grafts. Smaller tears occurred in 10 (7.9%) of the pseudophakic donor grafts and in 55 (6.1%) of the phakic donor grafts (p=0.476).
Endothelial cell density
Matching the recipients of pseudophakic donor grafts with recipients of phakic donor grafts resulted in balanced groups (table 2). At surgery, the average ECD in the pseudophakic donor group was lower than in the phakic donor group (table 2, figure 1). At 3 months after surgery, the drop in ECD was higher in the pseudophakic group than in the phakic group (figure 1, table 3). When controlling for confounder (donor age and cultivation time), the rate of ECL was 301 cells/mm2 (95% CI 106 to 497, p=0.003) higher in the pseudophakic donor grafts than in the phakic grafts. This meant that the difference in ECD between both groups increased (table 3). Beyond 3 months after surgery, no major differences in the rate of ECL were observed and ECD decreased at a similar rate between the two groups over the 36-month observation period (figure 1, table 3).
Baseline characteristics of DMEK recipients stratified by donor lens status
Mean endothelial cell loss and mean difference in endothelial cell density in cells/mm2 between pseudophakic and phakic donors after surgery
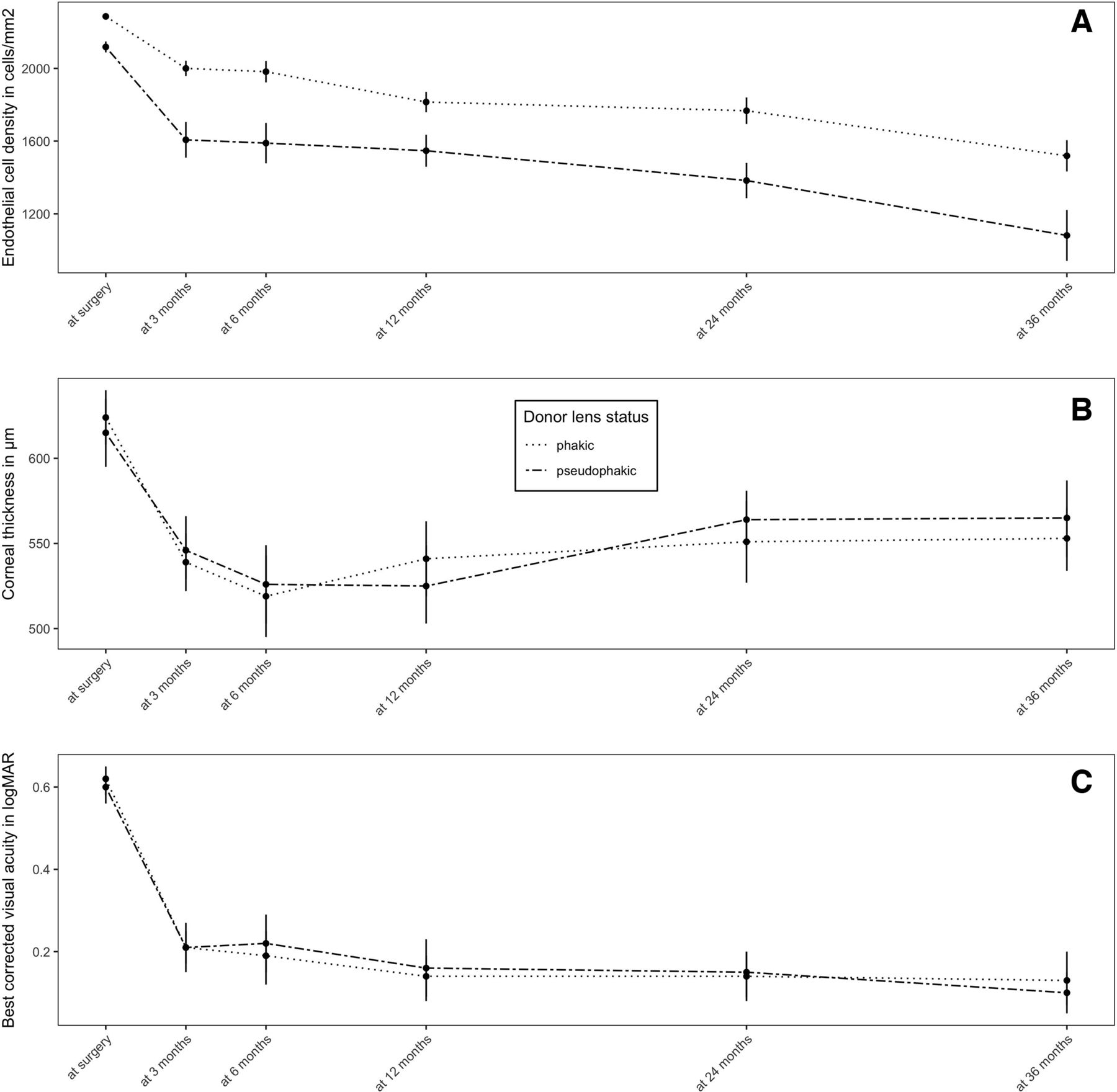
{kind=link}
Endothelial cell density (A), corneal thickness (B), and best corrected visual acuity (BCVA) (C) in recipients of phakic and pseudophakic donor grafts from surgery to 3 years after surgery.
BCVA and central corneal thickness
A significant postoperative increase in visual acuity was noted in both groups (p<0.001) with no difference between pseudophakic and phakic donor grafts (figure 1). The increase was highest up until 3 months after surgery, thereafter only minor changes in visual acuity were noted. The increase in BCVA remained stable throughout the study period. Similarly, central corneal thickness (CCT) dropped strongly up until 6 months after surgery (p<0.001) without any differences between both groups (figure 1). As of 12 months after surgery, a slight increase in CCT was noted in both groups (figure 1).
Complication rates
No relevant intraoperative complications were noted. Surgery time was comparable between both groups (data not shown). All DMEK surgeries were performed according to our standard procedure and by the same surgeon (NT)
In the pseudophakic group 26 cases (30%) required a rebubbling, whereas in the phakic group 16 cases (19%) required rebubbling (p=0.08). A second rebubbling was needed in four cases (4.6%) of the pseudophakic donor grafts and in three cases (3.5%) of the phakic grafts (p=0.711). When controlling for donor age, pseudophakic donor grafts were not associated with a higher risk of graft detachment (p=0.536).
Primary graft failures were observed in one case in each group. These were successfully treated with a re-DMEK. Immune reactions were seen in three patients (3.5%) in the pseudophakic group and in two patients (2.3%) in the phakic group. All cases resolved during the course of follow-up.
Discussion
Grafts of pseudophakic donors have a lower initial ECD than grafts from phakic donors and they lose ECD quicker during cultivation and surgery. The lower ECD, however, does not affect the mid-term postoperative outcomes.
The lower ECD of pseudophakic donor grafts was consistent over the entire study period. Prior to surgery, pseudophakic donor grafts showed a lower ECD at recovery, and these grafts lost a higher number of endothelial cells during cultivation. Further investigation should therefore also focus on changes of endothelial cell morphology and endothelial cell necrosis during and prior to cultivation. This could be done using a systematic approach described by Feizi et al14 who used a grading based on morphological criteria to explore the effect of donor features on postsurgical outcomes in patients undergoing deep anterior lamellar keratoplasty. Although Feizi et al14 did not find that morphological criteria were associated with worse postsurgical outcomes they might be correlated with the amount of ECL.
The higher loss in ECD in the pseudophakic group was independent of donor age and cultivation time. This suggests that prior exposure to cataract surgery renders donor grafts more susceptible to ECL during cultivation. We found that after cultivation, the average pseudophakic donor cornea was below the quality cut-off for an elective graft (at this clinic 2000 cells/mm2) whereas the average phakic donor exceeded it considerably. In fact, the rate of corneas with insufficient ECD was almost four times higher in the pseudophakic group than in the phakic group. This could mean that with a higher number of pseudophakic donors, cornea banks will have to increase the number of corneas recovered to achieve an equal number of high-quality corneas.
Besides an adequate ECD, suitability for graft lamella preparation is an additional aspect in DMEK surgery. Here we found that pseudophakic donor grafts were associated with a higher risk of preparation failure. This observation is different from a study by Schaub et al.13 who noted no preparation failures. Although we were unable to access the medical history of the donor for this retrospective study to account for diabetes status of the donor, a risk factor for preparation failure,15 we did control for complicating factors such as donor age and cultivation time.6 16 The higher rate of preparation failure suggests that adhesions following cataract surgery may contribute to complicating the preparation of pseudophakic donor tissue. New preparation techniques, as have been suggested for diabetic donor tissue,17 may help reduce preparation failure rates.
Although only corneas with an ECD ≥2000 cells/mm2 were transplanted, donor grafts from pseudophakic and phakic donors are not of the same quality. Consistent with previous studies,13 pseudophakic donor grafts have a lower ECD than phakic donor grafts at surgery. It has been suggested that donor age affects ECD negatively,8 but in our analysis the difference in ECD was independent of age and cultivation time. Similarly, Schaub et al.13 did not find an effect of donor age on ECD but they observed a strong effect of donor lens status. In addition, we show that immediately after surgery, but not during the remaining observation period, ECD drops considerably faster in pseudophakic donor grafts than in phakic grafts. This difference was not explained by possible confounders included in this study and could indicate that grafts from pseudophakic donors are more prone to ECL during surgery than grafts of phakic donors.
ECL can be influenced by many factors. In this study we had limited information on donor characteristics that could have affected ECD. Although some evidence suggests that a systemic disease such as diabetes does not affect ECD of donor grafts,15 this effect could be different for other diseases. We could not explore such effects and hence our interpretation is limited. On the other hand, postmortem time, cultivation time and donor age have been suggested to negatively affect ECD7 and were controlled for in our analysis. In addition, some studies suggest that recipient characteristics may be of greater importance for postoperative outcomes.15 We matched on known confounders such as age and diabetes and also included unknown ones such as use of antiglaucoma eye-drops.
Despite the difference in ECD, BCVA and CCT did not differ between pseudophakic and phakic donor grafts. This observation is similar to findings produced by Schaub et al.13 who suggest that resolution of corneal oedema may be faster in phakic donor grafts but that visual acuity is similar in both groups. Here we found almost no difference in the resolution of corneal oedema or increase in visual acuity. This indicates that although ECD differs between the two groups, up to 3 years after surgery, ECD levels in both groups are high enough to assure normal function.
Graft detachment is a frequent complication in DMEK surgery. To date, little is known about donor characteristic that could affect graft detachment. While some studies suggest that younger donor age is associated with a higher rebubbling rate,7 others indicate the opposite.10 It has been suggested that grafts from pseudophakic donors are more fragile or stiffer and could therefore be more prone to graft detachment.13 In this study, however, we did not find evidence for an effect of donor lens status on graft detachment.
In conclusion, pseudophakic donor grafts have a lower ECD and are more prone to ECL during cultivation and surgery. If recovering pseudophakic donor grafts becomes more common, cornea banks may have to increase their recovery rate in order to compensate for the lower quality of the grafts. In addition, surgeons should take special care when handling pseudophakic donor tissue as the risk of preparation failure can be higher than in phakic donor grafts. Although functional results of both grafts are comparable, long-term follow-ups are needed to compare the rate of graft failure between recipients of pseudophakic and phakic donor grafts.
Acknowledgments
We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Funds of Charité – Universitätsmedizin Berlin.
Footnotes
Contributors DP conducted the study, performed the analysis and wrote the first draft of the manuscript. AKBM and JS contributed to the analysis and interpretation of the findings and added to the writing of the manuscript. DP and JS conceived the study. NT performed the surgeries, interpreted the findings and contributed to the writing of the final manuscript. DP, JS and NT act as guarantors for the overall content of this work.
Funding DP is a participant in the BIH Charité Clinician Scientist Program funded by the Charité-Universitätsmedizin Berlin and the Berlin Institute of Health.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study obtained ethical clearance by the Charité Ethical Committee (EA4/167/16).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.