Article Text

Abstract
Objectives Two hundred thousand children worldwide are blind from cataract. Late presentation for surgery resulting in poor visual outcomes is a problem globally. We aimed to explore the reasons why children are not brought earlier for surgery in Nepal.
Methods and analysis Mixed-method study of carers of children with bilateral cataract attending a large non-government eye hospital were administered a proforma. A random sample took part in semistructured interviews and focus group discussions.
Results Carers of 102 children completed proformas; 10 interviews and 2 focus group discussions were held. 80.4% were Indian, 35.3% of children were female, and their mean age was 58 months (range 4 months to 10 years). Median delay in time between the carer first noticing a problem to presentation was 182 days IQR (60.8–364.8). This was significantly longer for girls (median 304 IQR (91.2–1094.4)) than boys (median 121.6 IQR (30.4–364.8); p=0.02). Cost to access care was a problem for 42 (41.2%) carers. 13 (12.8%) participants were not aware of treatment and 12 (11.8%) were aware but did not seek treatment. The community influenced carer’s health-seeking behaviour. Cataract was sometimes described as ‘phula’, meaning something white seen on the eye.
Conclusion Fewer girls presented for surgery, and they also had a significantly longer delay to presentation than boys. Carers are influenced by factors at family, community and socio-organisational levels. Approaches to increase timely access, particularly by girls, are required, such as health education using the term phula, which is widely understood.
- child health (paediatrics)
- eye (globe)
- lens and zonules
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Delay in presentation for cataract surgery resulting in poor visual outcomes is a problem in low-income countries.
Female children are less likely to undergo surgery for cataract than male children in many regions, particularly South Asia.
What are the new findings?
The time from the carer first noticing a problem with the child to presentation at the hospital for treatment was found to be significantly longer for female than for male children.
Members of the community were found to be an important influence on the health-seeking behaviours of carers.
The term ‘phula’ was used by some carers in interviews and focus group discussions to describe something white seen in/on the eye.
How might these results change the focus of research or clinical practice?
Outreach services that include active case finding of female children need to be employed.
Health education about phula, with an emphasis on seeking eye health services, may encourage access to eye care for serious eye conditions such as corneal ulcers and scars, and retinoblastoma.
Introduction
Worldwide an estimated 200 000 children are blind from cataract.1 Children with visually impairing cataract of early onset are at significant risk of visual deprivation amblyopia if surgery is delayed and/or optical correction and long-term follow-up are poor. Early cataract surgery with good follow-up is therefore crucial good visual outcomes. Delay in surgical treatment resulting in poor visual outcomes is a particular problem in low-income countries.2–4 Factors that lead parents or carers to delay seeking treatment for their child have been reported from India, Brazil, Nigeria and Tanzania (table 1), which can vary by location. Being an only child appeared to be a factor for earlier presentation in Brazil, but children who had a sibling presented earlier in India and Tanzania.1 5–7 In these studies, the sex of the child was not a factor affecting time to presentation for surgery. However, despite the incidence of cataract being equal in males and females, a systematic review showed that girls are less likely to undergo surgery in several regions, particularly in South Asia.8 In Nepal, only 26%9 and 30.8%10 of children undergoing surgery for bilateral cataract were female.
Reported causes of delay of presentation for cataract surgery from four different studies located in India, Nigeria, Brazil and Tanzania
In a study of carers of children undergoing surgery for cataract in India and China, despite lower surgical costs in India and similar distances to travel for care, children in India presented a year or more later than in China. The authors hypothesised that the greater delay in the Indian population could be due to lower rates of maternal work outside the home, tendency to rely on other family members for medical advice and greater likelihood of having to borrow money to cover hospital expenses’.11 The purpose of this study was to identify and explore factors influencing the health-seeking behaviour of carers of young children with cataract presenting to a tertiary eye hospital in rural Nepal.
Materials and methods
Congenital cataract was defined as cataract presenting within the first year of life with or without nystagmus, or after 1 year with nystagmus. Developmental cataract was defined as cataract presenting after 1 year of life without nystagmus. Delay in presentation was calculated using the time between the carer recognising a problem and date of presentation to Sagarmatha Choudhary Eye Hospital (SCEH).
Study site and design
A mixed-method cross-sectional study was conducted at SCEH in rural Nepal, located close to the Indian/Nepalese border. SCEH performed 766 paediatric cataract surgeries in 2017. All children receiving cataract surgery stay in the hospital for several days before and after surgery. Surgical fees can be waived for very poor patients.
Sample selection
Consecutive sampling was used where all carers bringing a child aged <10 years with bilateral congenital/developmental cataract during a 2-month period in June–August 2018 were eligible for recruitment. Children with unilateral cataract or cataract secondary to other causes (eg, trauma, uveitis) were excluded.
Ten carers from among those eligible were randomly selected to participate in semistructured interviews. One carer was selected every 2 days until 10 carers had agreed and were interviewed. Carers were interviewed while their child was awaiting surgery/postoperatively to avoid access bias. A further 7 (3 and 4) carers were selected in the same manner to take part in two focus group discussions (FGDs).
Data collection
Recruitment and data collection were conducted by a trained senior optometrist fluent in the local languages (Nepali, Hindi and Maithali).
Questionnaires
A data collection proforma, which was developed based on a literature review, was administered to carers (usually parents) of all children recruited by a senior optometrist. The following data were sought: their sociodemographic status, number of children and family history of childhood cataract. The distance between their place of residence and the hospital was calculated using a Global Positioning System mapping system. The visual function of each child and the presence of ocular/systemic comorbidities were assessed. The time interval between when the problem was first noticed to presentation at the hospital, and carer health-seeking behaviour during this time were recorded. Carers were asked who they first consulted, problems faced when accessing care and the direct and indirect costs of attending for surgery. Costs included for travel, accommodation and meals, hospital registration fees and for surgery, and general anaesthesia, if required. Inbound travel costs were doubled to estimate the total travel costs.
Semistructured interviews and FGDs
In the interviews and FDGs, the journey from identification of the cataract to presentation for surgery was explored using open questions supplemented with probing statements to guide discussion. The questions explored responses given in the proforma, to gain contextual information on the reason for delaying attendance. In addition, questions explored carers’ ideas about the cause and treatment of cataract and the actions they undertook to access care. Carers were asked how external influences affected their health-seeking behaviour, the barriers they encountered and their experiences of the eye health services.
Data analysis
STATA V.15 was used to analyse quantitative data from the study proforma. Time to presentation was not normally distributed so non-parametric methods were adopted: the Wilcoxon rank-sum and Kruskal-Wallis tests were used to compare two, or three or more groups, respectively. Spearmans rank correlation was used to assess associations between time to presentation and the age of the child, distance and cost.
NVivo V.12 was used to assist with analysis of qualitative data. Repeated elements identified from interviews were coded under nodes which were reviewed multiple times to produce 32 subnodes under three main node themes.
Patient and public involvement statement
There was no public or patient involvement in the design or conduct of this study. Written informed consent in the local languages was obtained for all carers, including to record interviews and to use anonymous quotes.
Results
During the study period, 104 potentially eligible children attended the hospital. Two were excluded (one>10 years, one traumatic cataract), leaving 102 for analysis. Thirty-five (34.3%) were female and the mean age was 58±41.3 months (range 4 months to 10 years)(table 2). Fourteen children (13.7%) were judged able to navigate/walk without assistance. Eight children (7.9%) had a comorbidity and 15 (14.7%) had a sibling with cataract. Ten carers underwent semistructured interviews (of four girls, six boys) and seven took part in FDGs (of one girl, three boys and one girl, two males).
Sociodemographic data of children and carers
Analysis of the qualitative data from semistructured interviews and FGDs generated three main themes: (1) the carer’s ideas about cataract, and concerns about the effect on the child and the family; (2) community influences on carer health-seeking behaviour and (3) healthcare care system factors influencing carer health-seeking behaviour.
Health-seeking behaviours of carers
Cataract was most frequently noticed by the mother (58.6%), followed by the father (16.2%), a grandparent (2.2%), sibling (1%), teacher (3%) or a health worker (2%). During interviews, no participant had a correct idea about the causes of cataract, even parents of children who had previously had cataract. However, many felt the problem could be resolved with medication. Four participants thought that the cataract was a normal occurrence or that it would resolve on its own. One carer reported a 4-year delay in seeking care as he believed no treatment was available.
Parents most went to see a local eye-care worker when they first noticed their child’s problem (43.1%), and 38.2% came directly to SCEH. However, in interviews, participants often reported consulting a neighbour or relative first. The relatives consulted were predominantly male. A positive opinion about the hospital from a community member encouraged participants to attend the hospital. Two participants reported that a community member identified the problem as cataract and advised them to go to an eye hospital for surgery. In four instances, incorrect advice was received from neighbours, relatives and community members which delayed health-seeking behaviour. This included advice to treat the child with eye drops, to consult a traditional healer or that the cataract would resolve on its own:
The child grows slowly and people in the community used to say that this is because of bad work I have done in a previous life. I spoke with my father in law and he said many children have this type of problem and it will go by itself. As time passed it was not becoming better, then I took the child to the doctor at the age of 4 months. I then came to know that this is cataract and needs surgery (Interview—Mother of a daughter)
In FDGs, the local term ‘phula’ was used. Staff at SCEH explained that this word is used to describe something white on or in the eye
I spoke first to my uncle when I noticed then I talked with my husband and he told me that this is a phula which will go by having drops. But it was increasing instead of decreasing, so I went to the doctor nearby in the village and the doctor diagnosed this as cataract (FGD—mother of a son).
Community members were an important source of support, most often through financial assistance. A lack of physical or moral support negatively influenced the health-seeking behaviours of some carers. ‘Nobody to bring the child’ was mentioned by four participants as a difficultly in accessing care.
Time from identification of cataract to presentation
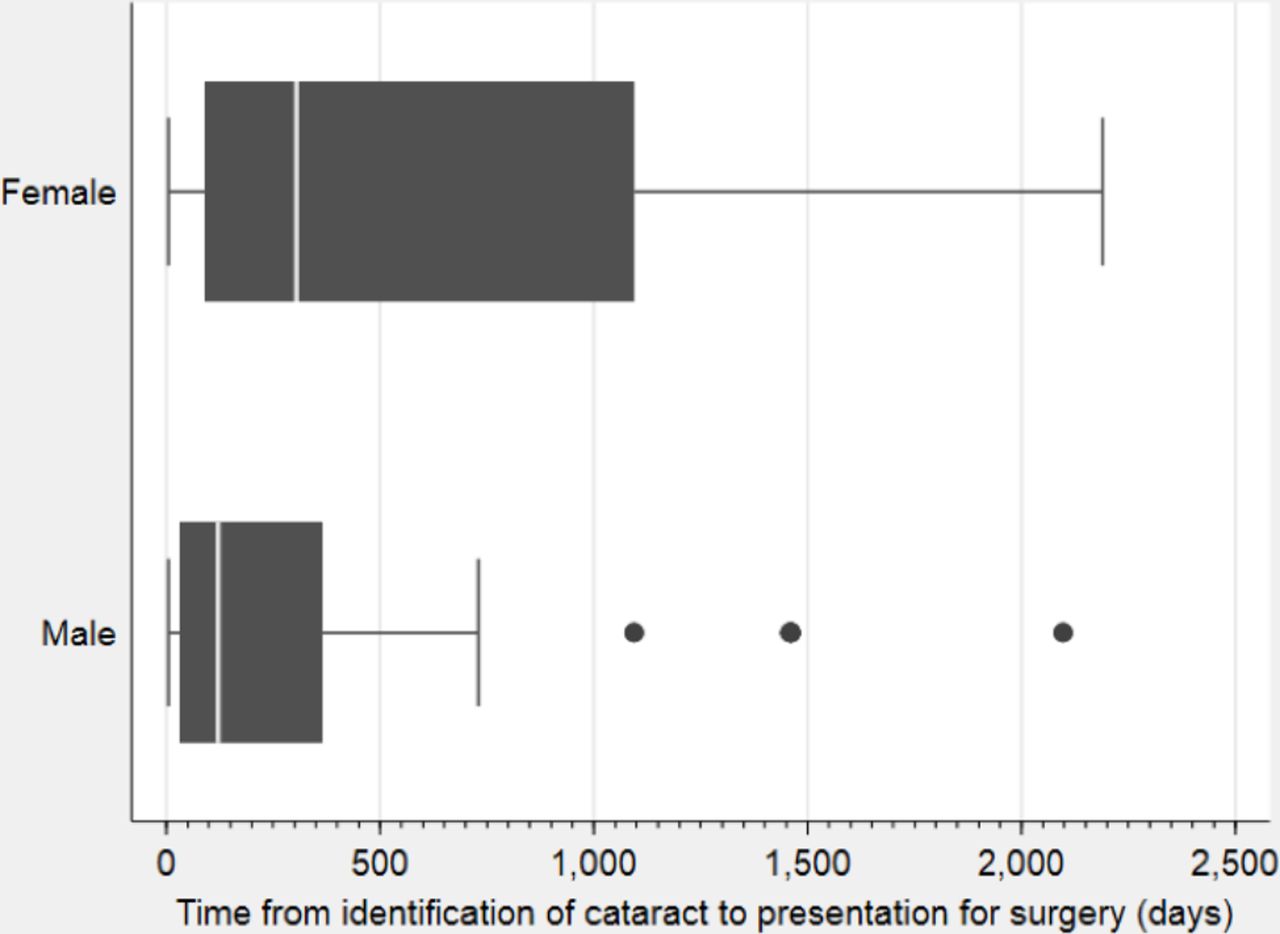
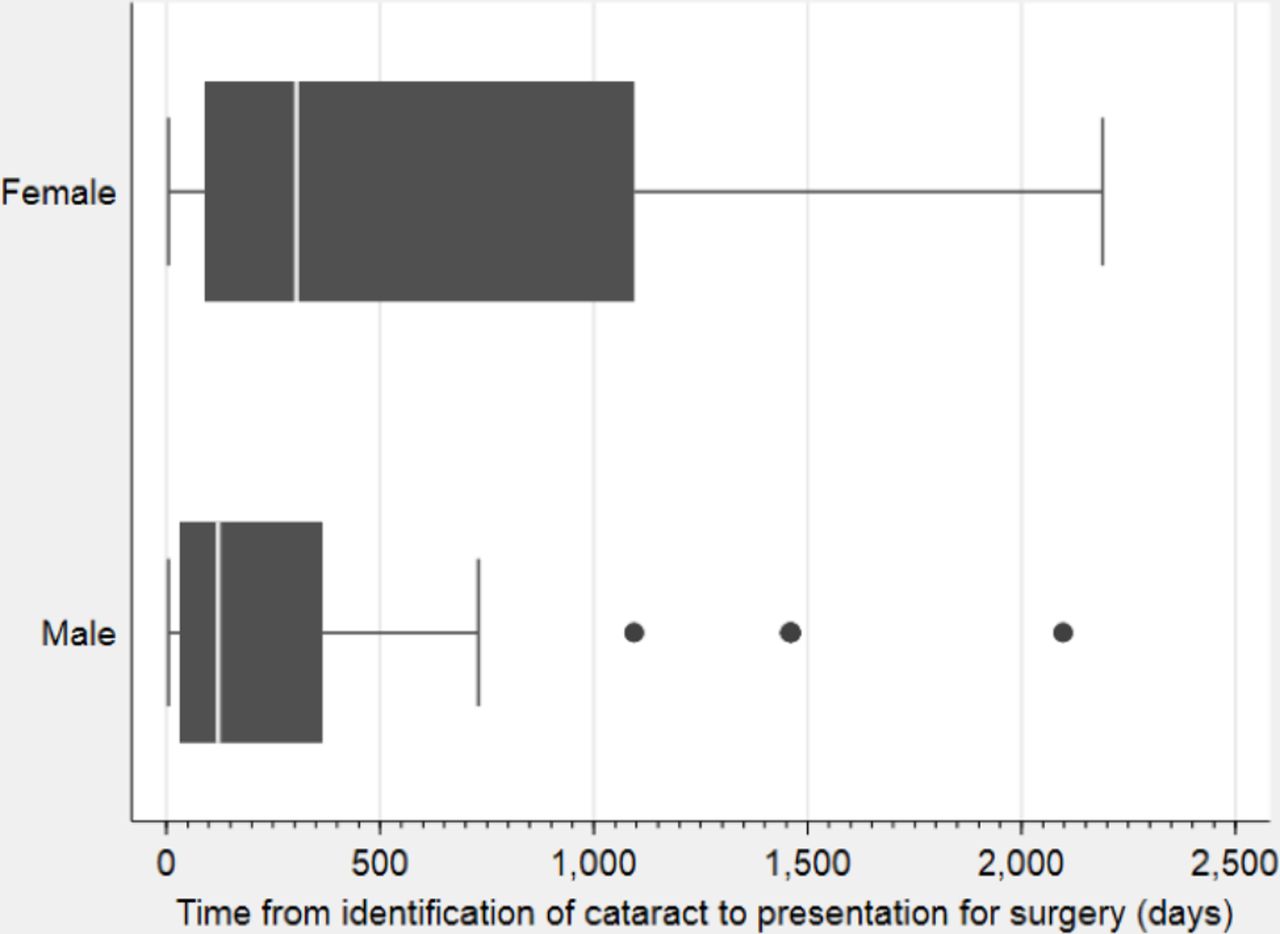
The median time to presentation was 182 days (IQR 60.8–364.8 days; figure 1) ranging from 5 days to 6 years. Only 19 (18.6%) children (29% of congenital cases) were brought before 1 year of age. There was a weak correlation between age of the child and time to presentation (r=0.35; see online supplementary figure S1).
Supplemental material
{kind=link}
Box plot of time from carer first realising a problem to attendance for surgery, by sex.
Girls presented significantly later than boys (median 304 and 121.6 days, respectively, p=0.02) after the carer first noticed a problem but there was no association between time to presentation and nationality, maternal or paternal literacy, educational status or occupation, cataract type or comorbidities (table 3). While not statistically significant, those with a sibling with cataract presented later on average than those without. In this group, approximately half (7) of the children were female.
Factors affecting time from realising a problem to attendance for surgery in days
The healthcare professional first consulted was not a factor influencing presentation (p=0.85) in either Indian (p=0.74) or Nepalese children (p=0.63). Participants lived on average 185.9 km from the hospital (range 24–748 km), but there was no correlation between distance (r 0.02) and time to presentation (see online supplementary figure S2). Although time to presentation was not significantly different between Indian and Nepalese participants, Indians lived almost 100 km further away from the hospital (p=0.003).
Supplemental material
Participants spent an average of 12 486.6 Nepalese rupees (US$110.50) to access surgical care. All but one family used public buses. 40.2% of participants used multiple modes of transport. There was no evidence of a correlation between total costs and time to presentation (r -0.13) (see online supplementary figure S3).
Supplemental material
41.2% of participants indicated that the main problem they faced was the financial cost, which was corroborated in interviews. Several carers said they had to borrow money. Two carers explained the complex factors they needed to consider before deciding to attend the hospital. During interviews, three mothers (including the one above) stated the problem was an alcoholic husband and another three mothers said there was nobody to bring the child.
A mother of an affected son explained that her husband was an alcoholic and they also had three unmarried daughters whose marriages would need to be paid for. Another carer explained that they had girl twins with cataracts.
I have only one son after four daughters but he is very challenged due to his vision problems and the father is an alcoholic, and so I had to take support from the neighbours to come here…One daughter is married but still I have three daughters unmarried, I have five children (Interview—mother of a son)
The previous twin had one eye operated 10 months ago. There was a financial problem and floods so we did not come for the other eye. This time I did not bring the first twin as I cannot look after both children so I brought the second twin so that at least she can have one eye to see and then later on I will bring both for the second eye. (Interview—father of twin girls)
Other barriers were distance (9.8%), ‘time away from work’ (7.8%), ‘means of transport’ (5.8%), ‘not aware of the service’ (12.8%) and ‘need not felt’ (11.8%). The presence of outreach services, such as school camps and buses hired by organisations to provide free transport, was mentioned by some as positive influences on treatment-seeking behaviour.
Carers’ perceptions of the eye hospital were overwhelmingly positive. Two negative comments were made regarding the cost of treatment.
Discussion
In this study, the majority of cataracts were identified by family members and three-quarters of children were brought within a year of their carer noticing a problem. Although many had no idea what it was and no one had a correct idea about the cause, many believed that it could be resolved with treatment and this belief was a positive influence on health-seeking behaviour. Members of the community sometimes had a positive influence on the health-seeking process, but lack of community support or incorrect advice from powerful (usually male) members of the community sometimes negatively influenced health-seeking behaviour.
A family history of cataract did not affect time to presentation for surgery in other studies in India, Brazil or Tanzania (table 1). However, in this study, time to presentation was considerably higher for children with a sibling with cataract than without, which meant that despite parents probably noticing the cataract earlier, they still delayed travel until the child was older, or they did not have the money to pay for a second child to have surgery.
Fewer female children attended the hospital and they were brought later than their male counterparts. A similar finding was reported in a systematic review in which only 29.1% of children undergoing surgery for bilateral cataract in South Asia were female.8 This is likely to be due to social structures and cultural norms in which male children are considered more economically and socially valuable.12 This phenomenon is best illustrated in this study by the mother of an only son with cataracts who was concerned about the financial burden of having to pay for weddings for multiple daughters. In rural communities, sons often grow up to become the primary source of family income, and daughters usually leave the family home after marriage. This means that heads of poor households face difficult decisions on how to allocate their scarce resources for healthcare.
Cost was the most frequently reported barrier to accessing healthcare, as was reported in a study comparing Chinese and Indian carer’s perceptions of cost in which only 2.5% of Indian carers reported cost not a problem.11 In 2010, 15% of Nepal’s population lived below the World Bank’s poverty line for low-income countries (ie, US$1.90 day). Accessing the funds for surgery (mean of US$110.50 in this study) would be problematic for many, as it represents almost 2 month’s household expenditure. Carers often reported seeking financial assistance from relatives and community members. SCEH provides discretionary services at no cost to some patients, including food vouchers, free accommodation for the family and part or full payment of all surgical costs. These services are likely to have influenced reported costs and explain the lack of correlation between cost and time to presentation.
Although not directly asked, three participants disclosed that their husband was an alcoholic, which was an unexpected finding. On all occasions, this information was volunteered while discussing the problems they had encountered to attend the hospital. However, in this study, a large proportion of participants were from Bihar, northern India, where high levels of alcohol abuse have been reported, including among rural agricultural workers. This led a state-wide ban on alcohol in 2016.13 14
In this study, several participants referred to the local term phula, which translates as ‘white eye’ in local languages. Corneal opacities are more common than cataract in this region,15 mainly from vitamin A deficiency and trauma. Communities are, therefore, more likely to have experience of corneal opacity, and be aware that corneal scars cannot be treated, which is likely to have influenced health seeking behaviour. Using phula in health education, including for influential community members, may positively influence health-related decision-making and presentation for treatment.
A limitation of this study was that it was based on an eye hospital, thus selecting for carers who had already made the decision to seek care. A further limitation is that for some questions, social desirability may have influenced response. Future studies need to focus on children with bilateral cataract in the community who have never accessed care.
In this study, we chose to measure the time interval between when carers first noticed the problem to when they presented. However, this is likely to be influenced by recall bias which may have led to misclassification of the type of cataract.
Financial cost is the most commonly reported factor leading carers to delay seeking treatment for their child with cataract and there is a lack of awareness of cataract in the community. Ideally, all eye surgery for children should be provided at no cost, as a means of increasing access and universal coverage for eye health in children. Surgery for both eyes during the same admission, either simultaneous or sequential, should be also considered, to eliminate the financial and distance barriers of accessing care twice, as has been used in several studies for childhood cataract and other eye conditions.16–18 This would have the additional advantage of reducing dense amblyopia in the second eye.
Gender inequity in the proportion of female children presenting for surgery and the time to presentation for cataract surgery is a major issue, probably reflecting the lower social status of females. Adult male members of the community also appear to be influential in decision-making about healthcare for children. Structural change that allows the empowerment of women in society is required to address this.
Better integration of eye care into general health services for children, with red reflex testing within 6 weeks of birth and child vision screening in primary health centres, would promote the early identification of children with cataract. Health education about phula, with an emphasis on seeking eye health services, may also encourage access to eye care for other serious eye conditions such as corneal ulcers and scars, and retinoblastoma. Outreach services that include active case finding of female children could also be employed.19
References
Footnotes
Contributors SJB and TS conducted the study. CB helped analyse the data. SKS supervised the study. CB and CG helped plan the study. AF supervised the study.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests CB is partly funded/supported by the National Institute for Health Research Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’ College London.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from the ethics committees of the London School of Hygiene & Tropical Medicine and SCEH.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.