Article Text

Abstract
Objective To prospectively explore the following patient-reported outcome measures (PROMs) in the management of neovascular age-related macular degeneration (nAMD): (1) self-reported visual function, (2) symptom-state, (3) general-health and (4) satisfaction of treatment.
Methods and analysis Corresponding to the four PROMs, participants responded to the following questionnaires: (1) National Eye Institute Visual-Functioning-Questionnaire (NEI-VFQ-25), (2) Patient-Acceptable-Symptom-Status (PASS 5), (3) EuroQol-Group-Questionnaire (EQ-5D-3L) and (4) Dimensions of Importance in Treatment of nAMD (DITAMD). Data were collected at baseline and after 3, 6 and 12 months of intravitreal antivascular endothelial growth factor treatment. Results were evaluated with t-tests and mixed linear regression analyses.
Results The study included 197 patients. At baseline NEI-VFQ-25 (79.53±14.52) and EQ-5D (0.74±0.28) had relatively high scores, whereas PASS 5 was below ‘acceptable’ (3.30±0.80). At 12 months NEI-VFQ-25 and PASS 5 showed significant improvement, whereas EQ-5D and DITAMD remained unchanged. At baseline patients receiving treatment of the better-seeing eye (BSE) (n=52) reported significantly worse NEI-VFQ-25 and PASS 5 than patients for whom treatment only involved the worse-seeing eye (WSE), (n=145). In contrast to BSE patients, there was no improvement of NEI-VFQ-25 for WSE patients at 12 months, despite a significant improvement in best-corrected visual acuity (BCVA). Two independent variables, treatment including the BSE and BCVA for the treated eye, were found to predict both NEI-VFQ-25 and PASS 5.
Conclusion After 12 months of nAMD treatment, there was a significant improvement in PASS 5 and NEI-VFQ-25, the latter depending on whether therapy included BSE. EQ-5D and DITAMD remained unaltered.
- macula
- retina
- vision
- visual perception
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of the study
What is already known about this subject?
Patient-reported outcome measures (PROMs) are increasingly emphasised in clinical research as a crucial part of neovascular age-related macular degeneration (nAMD) management. Yet, few studies on nAMD treatment define PROMs as the primary outcome.
What are the new findings?
The present study explored the performances of four different PROMs questionnaires in the assessment of nAMD patients during their first year of antivascular endothelial growth factor treatment. At baseline two of the PROMs questionnaires, self-reported visual function and general health, had relatively high scores, whereas visual symptom-state was under ‘acceptable’. Both self-reported visual function and symptom-state significantly improved during 12 months follow-up, with treatment including better-seeing eye and best-corrected visual acuity of the treated eye as main predictors.
How might these results change the focus of research or clinical practice?
Utilising appropriate PROMs tools in a multimodal approach to the management of nAMD could increase the understanding of how the disease and its treatment affect patients and reinforce a patient-centred care.
Introduction
Age-related macular degeneration (AMD) is a common cause of vision loss in the elderly and poses an increasing global health challenge due to an ageing population.1–4 AMD can be divided into the atrophic type and the more aggressive neovascular type (nAMD). nAMD develops in 10%–15% of patients, but it accounts for more than 80% of legally blind cases and can have a devastating effect on vision-related quality of life.5 6 The introduction of intravitreal antivascular endothelial growth factor (anti-VEGF) treatment has resulted in a paradigm shift in the management and prognosis of nAMD.7–10 Still, there are important limitations associated with such therapy. Although nAMD is a chronic disease, the aim of anti-VEGF treatment is not to cure patients, but merely to suppress the disease’s neovascular activity. In consequence many years of repetitive intravitreal injections, as well as clinical assessments to monitor response, may be necessary.11–13
The chronicity and invasiveness of anti-VEGF therapy makes it crucial to correlate treatment effects in terms of visual and anatomical changes to self-reported visual function and the patient’s own treatment experience.14–19 Such patient-reported outcome measures (PROMs) are emphasised in both clinical research and practice, and they are crucial in the evaluation of nAMD treatment.20–22 PROMs appraises the patient’s perspective of the disease, subjective treatment outcome and self-reported visual function.14 18 Various ophthalmic PROMs have been developed and studied among AMD patients,14 18 yet only a small proportion of studies on nAMD treatment include PROMs as primary outcome.23 In everyday clinical practice little attention is also paid to the correlation between visual acuity and disability as well as patient’s own treatment experience.6 24 Utilising several PROMs tools in a multimodal approach to the management of nAMD might increase the understanding of how the disease and its treatment affect patients.
Preserving visual function in daily life is a vital treatment goal for nAMD patients.16–18 From the clinician’s perspective functional outcome in terms of best-corrected visual acuity (BCVA) is typically evaluated monocularly, and most definitions of visual impairment focus on the status of the better-seeing eye (BSE). However, patients respond to PROMs based on their binocular vision, and it is challenging to assess how much each eye contributes to the self-reported visual function.25 Especially for eye diseases affecting the central vision (eg, AMD), there are conflicting data regarding the relationship between BCVA of the worse-seeing eye (WSE) and self-reported visual function.26 The choice of PROM instrument is also of importance in capturing the influence of the BSE or WSE.25
The aim of the present study was to prospectively explore how newly diagnosed nAMD patients responded to four different PROMs that focus on self-reported visual function, general health, acceptable visual symptom-state and satisfaction of anti-VEGF treatment during 12 months of follow-up. Furthermore, we wanted to explore which factors influence these PROMs instruments and to compare the responses of patients for whom treatment included BSE with the responses of patients that only received treatment of the WSE.
Materials and methods
The study included treatment-naïve nAMD patients scheduled to initiate intravitreal anti-VEGF therapy at the Department of Ophthalmology, Oslo University Hospital, Norway. The inclusion period was from February 2015 to March 2017. Inclusion criteria were Scandinavian-speaking patients without known cognitive impairment that were scheduled for intravitreal treatment. Treatment was in accordance with the department’s clinical practice; bevacizumab (Avastin; Roche, Basel, Switzerland) was the first-line drug, while treatment-resistant eyes defined as those with the inability to achieve full resolution of macular fluid despite monthly bevacizumab injections, were converted to aflibercept (Eylea; Bayer, Leverkusen, Germany). Injection intervals were individualised by means of a treat and extend (T&E) algorithm27; if a dry macula was achieved, the treatment frequency was extended at 2-week intervals until a 12-week interval was reached or macular fluid reoccurred on optical coherence tomography. Researchers that were not involved in the diagnostic or therapeutic intervention carried out the recruitment procedure and data collection.
Data collection
Patients responded to PROMs at baseline and at 3, 6 and 12 months (with the exception of the questionnaire measuring satisfaction of treatment, for which baseline was not applicable). At baseline the data collection took place as a face-to-face interview in the department’s outpatient clinic at the time of diagnoses and indication for treatment (prior to first injection), while telephone interviews were conducted for the follow-up evaluations. The following four PROMs were used:
The National Eye Institute Visual Functioning Questionnaire-25 (NEI-VFQ-25) is a vision-specific inquiry.28 It contains 25 questions on visual function in daily life, is sensitive to changes in visual acuity and commonly used in AMD studies as well as proven to correlate with visual acuity in treatment of nAMD.29 The score ranges from 0 to 100; 0 designates worst state and 100 designates no disability related to visual function. NEI-VFQ-25 has 12 subcategories: (1) general health; (2) general vision; (3) ocular pain; (4) near vision; (5) distance vision; (6) social functioning; (7) mental health; (8) role difficulties; (9) dependency; (10) driving; (11) colour vision; (12) peripheral vision.
Dimensions of Importance in Treatment of neovascular Age-related Macular Degeneration (DITAMD) is a questionnaire measuring the satisfaction of important dimensions during intravitreal injection treatment.30 DITAMD contains 15 dimensions: (1) receive treatment to preserve vision; (2) information about your diagnosis and treatment; (3) waiting time at the clinic; (4) trust in those treating you; (5) accommodating staff; (6) follow-up structure; (7) planning of treatment consultations; (8) treatment continuity; (9) good pain relief during injection treatment; (10) injection technique to reduce discomfort during treatment; (11) transport/travel challenges back and forth from the eye clinic; (12) good hygiene during treatment; (13) receive early access to treatment after referral; (14) involvement in treatment decisions; (15) information about possible visual aids. DITAMD has a weighted algorithm to calculate the total score, which implies the relative importance among the dimensions. The score ranges from 1 to 5; 5 designates ‘best managed’ and 1 designates ‘not at all managed’.
Patient Acceptable Symptom Status (PASS 5) contains a simple question measuring the patient’s symptom state. In the current study the question specifically regarded visual symptoms during the last month. The score ranges from 1 to 5; 5 designates ‘very bad’ and 1 designates ‘very good’.31
The EuroQol Group Questionnaire (EQ-5D-3L) evaluates the patient’s self-rated health. EQ-5D-3L contains five questions: (1) mobility; (2) self-care; (3) usual activities; (4) pain/discomfort; (5) anxiety/depression with three response options. The total score ranges from 0 to 1; 0 designates ‘dead’ and 1 designates ‘perfect health’.32
In addition, the following clinical data were collected from the patients’ medical records: BCVA for each eye, choice of anti-VEGF medication, and number of injections received in 12 months. BCVA was obtained from a ClearChart (Reichert Technologies, Depew, New York, USA) digital acuity test that displayed letter optotypes and logarithm of the minimal angle of resolution (logMAR) line size progression.
Patient and public involvement
Two patient research partners with known neovascular AMD (nAMD) were involved in the planning of the study. They gave comments and advice regarding study information and questionnaires. One of the four questionnaires used in the study, DITAMD, was developed in partnership with nAMD patients.30 Patients that responded to the questionnaires in current study also gave their opinion on the relevance of each questionnaire. Finally, preliminary study results have been presented for patients and their relatives as part of the clinic’s patient education programme.
Statistical analyses
Paired sample t-tests were used to examine changes in PROMs and BCVA from baseline to 12 months; for NEI-VFQ-25 the analyses included its subscores. In order to relate PROMs to treatment of either the BSE or WSE, we defined two patient subgroups: (1) patients for whom anti-VEGF treatment included the BSE, as defined by BCVA (the subgroup also contained patients receiving bilateral treatment) and (2) patients for whom treatment only included the WSE. Independent sample t-tests were used to compare the BSE and WSE subgroups.
Regression analyses with mixed linear models were used to examine the influence of independent variables on PROMs during follow-up. We also performed subscore analysis of NEI-VFQ-25 ‘near vision’, since this subscore is strongly associated with central vision. The independent variables included in the regression analyses were: age, gender, number of injections, BCVA for the treated eye, BSE treated (yes/no) and bilateral treatment (yes/no). Statistical significance was defined as p<0.05. Data are presented as mean (±SD). Mixed models were performed using R (V.3.4.1) and the package lme4, all other analyses were performed using SPSS Statistics V.25.
Results
Of 203 naïve nAMD patients screened for participation, 197 were included in the study. Three patients declined and another three did not meet the inclusion criteria. Mean (SD) age was 83.4 (7.6) years and 140 (71%) were females. The mean BCVA was 0.59 (±0.51) logMAR for the treated eye and 0.19 (±0.26) logMAR for the best eye (table 1).
Baseline characteristics. All patients and patients divided in two subgroups: (1) treatment included the better seeing-eye (BSE) defined by best corrected visual acuity (BCVA) (the subgroup also contained patients receiving bilateral treatment) and (2) patients for which treatment only included the worse-seeing eye (WSE)
Baseline PROMs
The baseline PROMs values were generally high; mean NEI-VFQ-25 patient-reported visual function was 79.53 (±14.52) out of 100 and mean EQ-5D was 0.74 (±0.28) out of 1.0. In contrast, the baseline PASS 5 score was of 3.30±0.80 out of 5 (table 1).
The BSE subgroup (n=52) had a better mean baseline BCVA for the treated eye than the WSE subgroup (n=145) (table 1), and it reported significantly worse NEI-VFQ-25 and PASS 5 scores. There was no significant difference in baseline EQ-5D between the subgroups, but there was a trend towards lower values in the BSE subgroup.
Improvement of PROMs compared to BCVA during 12 months of treatment
During the 12 months follow-up, patients received a mean of 9.2 (±2.9) injections. The proportion of treatment resistant eyes that were converted to aflibercept was 8% at 3 months, 25% at 6 months and 48% at 12 months. There were no significant differences between the BSE and WSE subgroups for neither mean number of injections nor proportion of treatment resistant eyes converted to aflibercept (data not shown). The main reasons for discontinuing treatment at 12 months were permanent loss of BCVA (n=26), death (n=3) and personal choice (n=2). At 12 months 168 of 197 patients responded to the PROMs questionnaires.
There was a significant improvement in both BCVA (p<0.001) and NEI-VFQ-25 patient-reported visual function (p<0.05) at 12 months compared with baseline (table 2, figure 1). There was also a significant improvement in PASS 5 at 12 months compared with baseline, from ‘under acceptable’ (3.3) to ‘over acceptable’ (2.8). There were no significant changes in EQ-5D and DITAMD management scores (table 2).
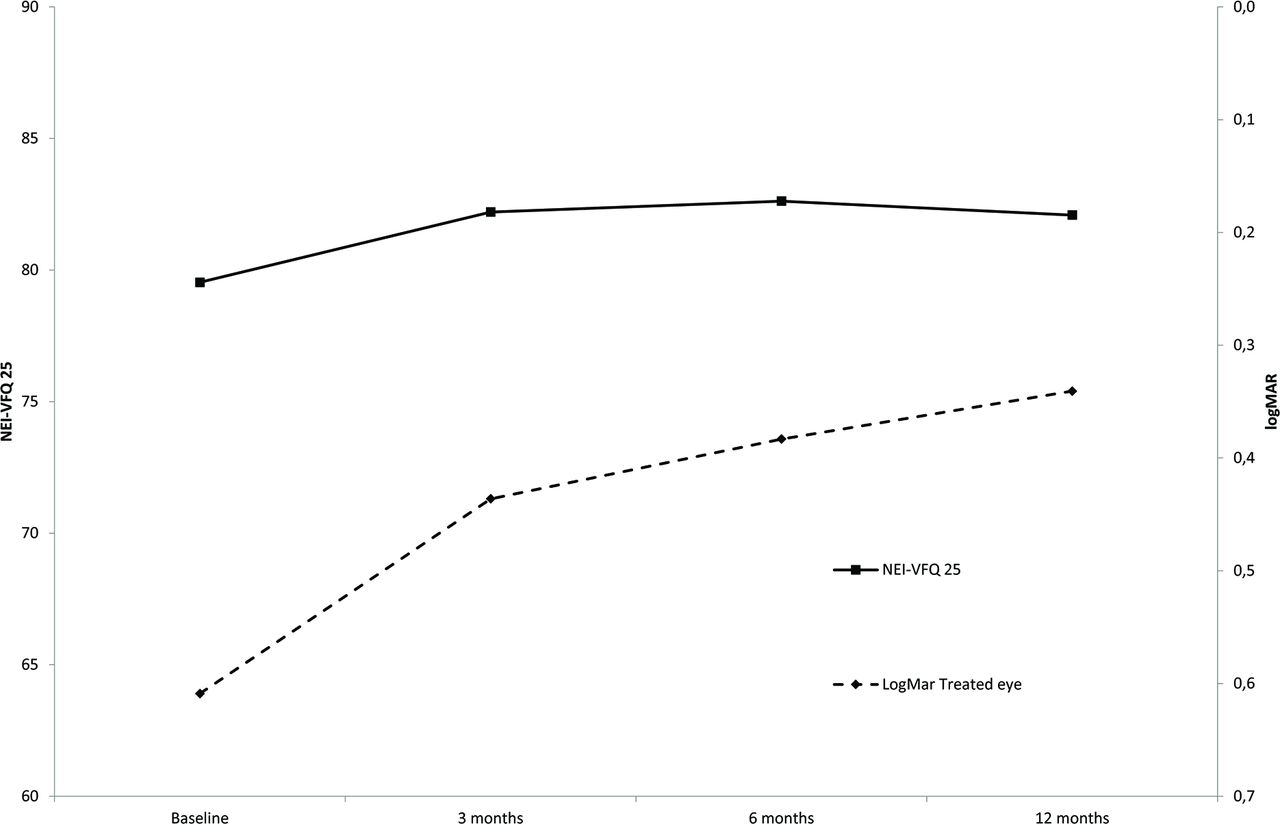
Relationship between self-reported visual function (NEI-VFQ-25) and best corrected visual acuity in logMAR of the treated eye during 12 months of antivascular endothelial growth factor therapy for all patients in the study. NEI-VFQ-25, National Eye Institute Visual-Functioning-Questionnaire-25.
Paired sample t-test analyses showing the change in patient reported outcome measures (PROMs) and best corrected visual acuity (BCVA) measured during 12 months follow-up for all patients and for the subgroups where treatment included better seeing-eye and patients for which treatment only included the worse-seeing eye
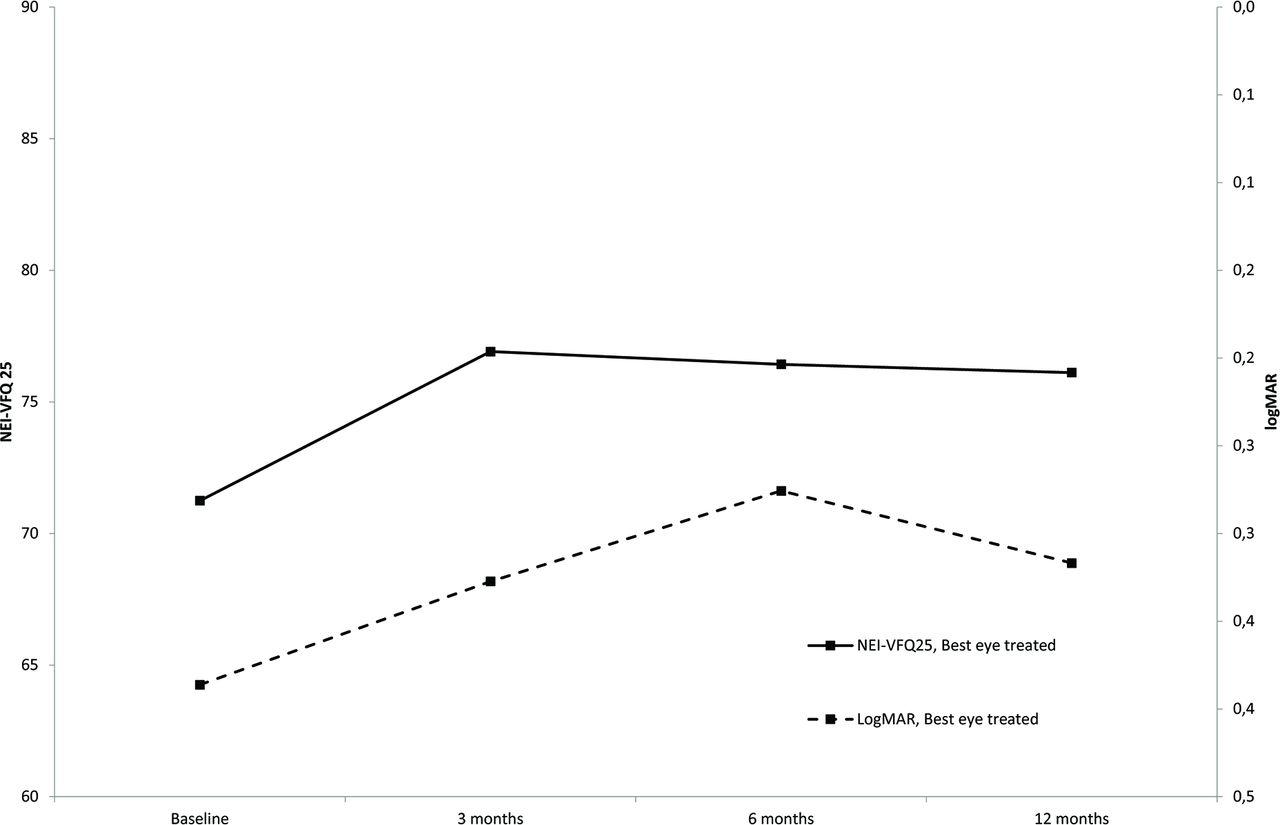
For the WSE subgroup there was no significant change in patient-reported visual function, despite a significant improvement in BCVA at all time-points (p<0.001) (table 2, figure 2, online supplementary table 1). The BSE subgroup only displayed a significant improvement in BCVA at 6 months (p<0.05) (table 2). Nevertheless, there was significant improvement in patient-reported visual function from baseline to both 3, 6 and 12 months (table 2; figure 3). Both WSE and BSE subgroups had a significant improvement in PASS 5 from baseline to 12 months, and both groups reported an ‘over acceptable’ state at 12 months (table 2). EQ-5 and DITAMD only displayed small, non-significant changes.
Supplemental material
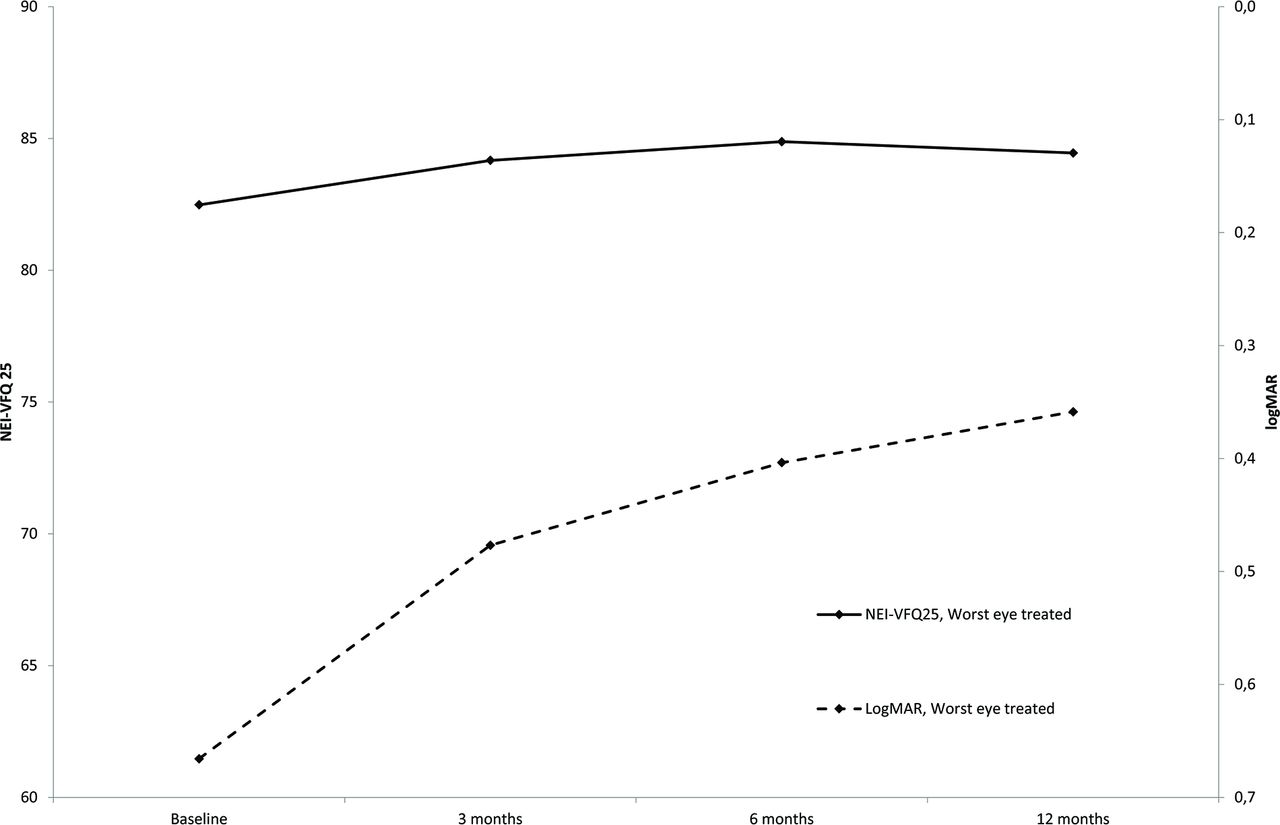
Change in self-reported visual function (NEI-VFQ-25) and best corrected visual acuity (BCVA) in logMAR of the treated eye during 12 months of follow-up for the subgroup where treatment only included the worse-seeing eye. The solid line represents NEI-VFQ-25, whereas the dotted line represents logMAR BCVA of the treated eye. NEI-VFQ-25, National Eye Institute Visual-Functioning-Questionnaire-25.
{kind=link}
{kind=link}
{kind=link}
Change in self-reported visual function (NEI-VFQ-25) and best corrected visual acuity (BCVA) in logMAR of treated eye during 12 months of follow-up for the subgroup where treatment included better seeing-eye. The solid line represents NEI-VFQ 25, whereas the dotted line represents logMAR BCVA of the treated eye. NEI-VFQ 25, National Eye Institute Visual-Functioning-Questionnaire-25.
Paired sample t-tests of NEI-VFQ-25 sub-scores showed a significant improvement after 12 months of treatment for the following sub-scores: “general vision”, “near vision”, and “mental health” (table 3). Analyses also showed a significant decrease in the sub-scores “general health” and “colour vision” (table 3).
Paired sample t-test analyses showing the change in points of NEI-VFQ-25 sub-scores from baseline to 12 months of antivascular endothelial growth factor treatment
Variables predicting PROMs during 12 months of treatment
Mixed linear regression analyses showed that among factors predicting PROMs response during the 12 months follow-up, both treatment including the BSE and BCVA of the treated eye were predictors of both self-reported visual function in general and its sub-score ‘near-vision’, as well as the visual symptom-state (online supplementary tables 2 and 4). We also found that gender predicted general health where; on average, men reported better health than women (online supplementary table 3). In addition, people who were treated on both eyes had higher general health. Furthermore, both age and follow-up time were found to predict satisfaction of treatment (online supplementary table 5). Finally, patients with higher treatment intensity had visual symptom-state improved; however, this effect decreased during the study period (online supplementary table 4).
Supplemental material
Supplemental material
Supplemental material
Discussion
The present study investigated how nAMD patients responded to four different PROMs during the first year of intravitreal anti-VEGF treatment. At baseline both self-reported visual function and general health values were high, whereas acceptable visual symptom-state was below ‘acceptable’. During 12 months of treatment, both symptom-state and self-reported visual function significantly improved, whereas general health and satisfaction of treatment remained unchanged. Interestingly, the patients that only received treatment of the WSE did not experience the same improvement in self-reported visual function as the patients for whom treatment included the BSE.
Patient demographics, general health-state, and the time from diagnosis to treatment may affect baseline self-reported visual function. The study setting was a large university clinic in a country with a universal public health system; national guidelines set a limit of 6 weeks from time of referral to initiation of nAMD treatment. We found that the overall NEI-VFQ-25 scores (79.5) were slightly higher than reported in the pivotal MARINA (69.3) and ANCHOR (69.9) nAMD trials, but somewhat lower than a recently published Swiss real-life study (86.5).29 33 Our patient population also had a higher mean age (83.4 years) than the respective studies (mean 77.1, 77.0 and 76.7 years).
Following initiation of intravitreal anti-VEGF treatment, nAMD patients will typically experience an initial improvement in BCVA before plateauing. The goal of anti-VEGF treatment in nAMD is principally a long-term stabilisation of neovascular disease and prevention of rapid vision loss.8 10 The present study found significant improvement in both BCVA and self-reported visual function at 12 months. In addition, BCVA of treated eye was found to be a predictor for self-reported visual function as well as visual symptom-state, confirming the association between the objective and subjective visual function and their mutual response to anti-VEGF treatment.29
Previous research suggests that a clinically meaningful change in PROMs varies by both population and context.34 A study of nAMD patients performed by Suñer and colleagues indicates that a 4-points to 6-points change in NEI VFQ-25 score, corresponding to a 15-letter change in BCVA, represents a minimal clinically important difference (MCID).29 In the present study the mean improvement in NEI-VFQ-25 at 12 months was 2.4 points, and only two NEI-VFQ-25 sub-scores (‘general vision’ and ‘mental health’) displayed a MCID of at least four points. Yet, for the BSE subgroup the mean overall improvement was 5.1 points at 12 months. Despite the absence of concurring improvement in BCVA, this satisfies the definition of a MCID in self-reported visual function. Notwithstanding an improvement in BCVA of more than 15 letters at 12 months, patients that only received treatment of the WSE did not experience a similar improvement in self-reported visual function. Treatment including BSE was also found to be a predictor for self-reported visual function in general, the subscore ‘near-vision’, as well as visual symptom-state during 12 months of treatment. These findings support the notion that treatment including the BSE more profoundly affects the self-reported visual function.23 In the present study a ceiling effect due to higher baseline PROMs scores for the WSE subgroup may have confined the potential for PROMs improvement. By contrast, previous studies have shown a correlation between self-reported quality of life and BCVA, regardless of treatment of WSE or BSE.25 26 For instance, in the MARINA and ANCHOR trials, NEI-VFQ-25 improved in both the BSE and WSE subgroup. Nevertheless, the improvement in the WSE subgroup was only modest (2.6 points at 24 months) and did not satisfy the definition of a MCID.26
A clinical dilemma arises from the fact that patients whose WSE is being treated fail to report a clinically meaningful improvement in PROM. The finding raises the question as to which extent anti-VEGF treatment is of value in the perspective of a WSE patient. Still, we do not believe that lack of PROM improvement represents an argument against WSE treatment. Instead, it underscores the importance of proper counselling of nAMD patients; an individual whose WSE is being treated should be informed that AMD inevitably contains a risk of bilateral neovascular involvement. In the event of visual loss in the second eye, the value of WSE treatment becomes apparent. Ultimately, disseminating PROMs knowledge in the follow-up of nAMD patients could help tailor counselling and treatment in line with individual expectations, thereby promoting a patient-cantered care.
There was also a significant improvement in PASS 5 from baseline to 12 months, corresponding to a visual symptom state improvement from ‘under acceptable’ to ‘over acceptable’. Accordingly, PASS 5, which composes only a single question about visual symptoms, can be used as a quantitative measurement of the patient-reported treatment effect. Beyond the NEI-VFQ-25 and PASS 5 questionnaires, a significant change in PROMs was not found. The observation adds to the evidence that EQ-5D, a generic PROM, is less sensitive to changes in visual function.35 Similar findings were recently reported in a glaucoma study.36 The lack of change in DITAMD management total score may indicate that this PROM merely points to patients’ experience with specific treatment dimensions and how they are managed, rather than recognising overall treatment alterations.30
The study has some important limitations. The number of patients in the BSE subgroup was smaller than in the WSE group, challenging the comparison between the two subgroups. Still, the two subgroups had similar age and gender distributions, as well as similar number of injections and drug of choice. Furthermore, the current definition of BSE and WSE was only based on the BCVA and did not include a cut-off limit, as others have suggested.26 Still, if a limit were to be defined as at least five letters,26 90.8% of the patients in our study would have had a clinical relevant difference in BCVA between the eyes.
In conclusion, among four different questionnaires evaluating patient-reported outcomes during 12 months of anti-VEGF treatment of nAMD, there was a significant improvement in PASS 5 and NEI-VFQ 25 scores, the latter being highly dependent on whether treatment included the BSE. The two remaining questionnaires, EQ-5D and DITAMD management did not display significant changes despite treatment.
Supplemental material
Acknowledgments
We are grateful for the research grant from the Norwegian Association of the Blind and Partially Sighted, The Norwegian Nurses Organization and Division of Head, Neck and Reconstructive Surgery at Oslo University Hospital. We appreciate the help we received from the administrative personnel, other health professionals and physicians at the medical retina unit who helped by identifying newly diagnosed patients. We are grateful to the patients who participated in the study. Finally, we thank the University of Oslo for hosting the PhD education and Oslo University Hospital for financial support.
References
Footnotes
TH and MCM are joint senior authors.
Funding The study was funded by the Norwegian Association of the Blind and Partially Sighted, The Norwegian Nurses Organization and Division of Head, Neck and Reconstructive Surgery at Oslo University Hospital.
Competing interests ØKJ has received lecture fees from Allergan, Alcon and Bayer, has been a member of a Bayer advisory board and an investigator in an Alcon sponsored clinical trial. MCM is member of Bayer and Novartis advisory boards and is an investigator in an Alcon sponsored clinical trial.
Patient consent for publication Written informed consent was obtained before inclusion.
Ethics approval The study adhered to the Declaration of Helsinki and was approved by the Regional Committee for Medical and Health Research Ethics (ID: 2014/1523) and the Institutional data protection officer.
Provenance and peer review Not commissioned; externally peer reviewed.