Article Text

Abstract
Objective To report four cases of new onset or exacerbation of uveitis following administration of infliximab.
Methods This retrospective observational case series includes four patients who developed new onset or exacerbation of uveitis paradoxically during infliximab treatment.
Results Four patients were assessed, including three women, with a mean age of 33 (14–84) years. Infliximab was introduced for the treatment of scleritis associated with rheumatoid arthritis (two cases), chronic anterior uveitis associated with juvenile idiopathic arthritis (JIA) (one case) and Crohn’s disease (one case). Anterior scleritis associated with rheumatoid arthritis successfully improved following infliximab administration; however, macular oedema or dense vitritis paradoxically developed in two cases. In one case, infliximab was switched to tocilizumab. In another case, infliximab was discontinued, and additional corticosteroids and immunosuppressive medications were added. In one patient with JIA, new-onset macular oedema and exacerbation of anterior uveitis were observed during infliximab treatment, so the patient was switched to adalimumab. In the patient with Crohn’s disease treated with infliximab, severe vasculitis and macular oedema occurred, requiring intravitreal triamcinolone injection. The patient was switched to adalimumab. Given that these reactions were paradoxical effects of infliximab, infliximab treatment was discontinued in all cases, and additional corticosteroids or immunosuppressive medications were added. All cases remained free of ocular inflammation at the last visit.
Conclusion Uveitis rarely occurs de novo or is exacerbated during infliximab treatment. Cessation of infliximab led to resolution of this paradoxical adverse effect.
- infliximab
- tumour necrosis factor
- uveitis
- paradoxical effects
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Paradoxical ocular inflammation in response to tumour necrosis factor (TNF) inhibitors has been mainly observed with etanercept. Other TNF inhibitors, such as infliximab and adalimumab, can also induce paradoxical adverse events. However, the details regarding the type of uveitis and clinical course were not yet reported.
What are the new findings?
We reported the clinical course of four cases of new onset or exacerbation of uveitis following administration of infliximab. All cases developed or exhibited exacerbated posterior ocular inflammation. Cessation of infliximab led to resolution of this paradoxical adverse effect.
How might these results change the focus of research or clinical practice?
Ocular inflammation is paradoxically a potential adverse effect of infliximab. Patients being treated with infliximab should be closely monitored for the development of new uveitis.
Introduction
Sclerouveitis is presumed to have autoimmune origins and is frequently associated with systemic inflammatory conditions, such as rheumatoid arthritis (RA), ankylosing spondylitis, psoriasis and Crohn’s disease. Cases with anterior uveitis are typically treated with local therapy alone, but cases with posterior uveitis are often treated with systemic therapy. Treatment of severe uveitis requires a similar approach to systemic inflammatory conditions, namely corticosteroids, systemic immunomodulation agents and biologics. Tumour necrosis factor-α (TNF-α) plays a key role in ocular inflammation as demonstrated by animal studies1 and is detected in the ocular fluids of inflamed eyes in humans.2 Clinically, the use of TNF inhibitors has also been very successful in controlling ocular inflammation,3 4 although patients receiving TNF inhibitors are at high risk of infections and reactivation of latent tuberculosis infection and the overall risk of opportunistic infections should be considered before beginning a course of TNF inhibitors.5
Intriguingly, paradoxical adverse effects (PAE), which are defined as the onset or exacerbation of disorders that are typically improved by TNF inhibitors, have been reported.6–8 These paradoxical effects mainly include psoriasiform skin reaction, uveitis, inflammatory bowel disease, sarcoidosis and vasculitis. Paradoxical ocular inflammation in response to TNF inhibitors has been mainly observed with etanercept.9–11 Although less frequently, other TNF inhibitors, such as infliximab and adalimumab, can also induce paradoxical adverse events. Twenty-two cases of inflammatory eye disease have been reported to be associated with the use of infliximab for rheumatic disease or inflammatory bowel disease.9 10 12–14 However, details regarding the type of uveitis and clinical course were unclear in most cases. The aim of this article is to report four cases of new onset or exacerbation of uveitis following administration of infliximab.
Materials and methods
This retrospective study included four patients with new-onset or exacerbated uveitis following administration of infliximab who were followed up at Japan Community Health Care Organization (JCHO) Osaka Hospital in Japan.
The medical records of the patients were reviewed for demographic data (age and gender), ocular and systemic diagnoses, type of TNF inhibitors and dosage schedule, previous immunosuppressive therapies, concurrent drug usage, response to ocular and articular treatment, and ophthalmic findings (laterality, the location and degree of ocular inflammation, and visual acuity levels).
Patient and public involvement statement
Patients were not directly involved in the conception, design or interpretation of this study. However, we have a plan to disseminate this information widely to ophthalmologists and rheumatologists as well as potential patients.
Results
We identified four patients with new-onset or exacerbated uveitis following administration of infliximab as specified in table 1. Other than ocular PAEs, we experienced no systemic adverse effects in these four patients.
Cases of new-onset uveitis associated with infliximab
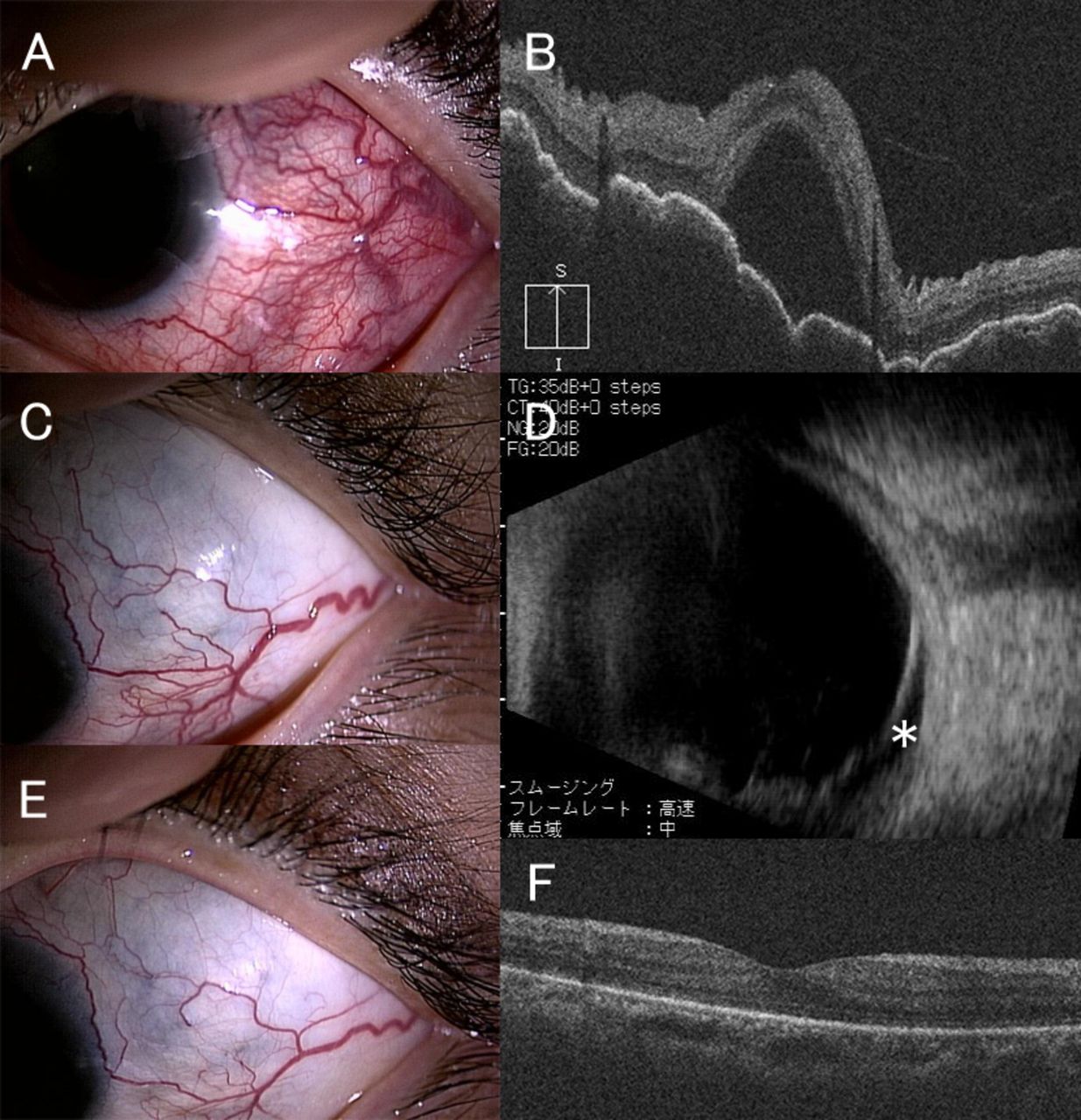
Patient 1. An 84-year-old woman with RA presented with redness in her left eye. Posterior inflammation was not observed, and she was diagnosed with anterior scleritis (figure 1A, B). She received etanercept therapy (25 mg twice weekly) in combination with 3 mg oral prednisolone treatment, and her articular symptoms remained in remission. Her visual acuity was 1.0 in the left eye with normal intraocular pressure. Given that scleritis is a potential adverse effect of etanercept, as previously reported, we decided to change the anti-TNF drug from etanercept to infliximab at 5 mg/kg. Four months after starting infliximab, scleritis improved (figure 1C), and her joint disease was also in remission. However, she complained of decreased vision in her left eye. Her visual acuity decreased to 0.15, and dilated fundal examination revealed macular oedema and vitreous opacity in the left eye (figure 1D). We added 40 mg oral prednisolone treatment to the infliximab treatment. However, posterior segment inflammation remained unchanged; therefore, we decided to switch infliximab to tocilizumab. One month after starting tocilizumab, both scleritis and macular oedema were completely resolved (figure 1E, F). To date, no flare-up of anterior and posterior scleritis has been noted for 12 months.

During etanercept therapy in patient 1 with rheumatoid arthritis, slit-lamp examination reveals scleral hyperaemia (A). Optical coherence tomography (OCT) reveals no evidence of macular oedema (B). Four months after switching to infliximab, the anterior scleritis improved (C); however, macular oedema occurred (D). After switching to tocilizumab, both scleritis and macular oedema were completely resolved (E, F).
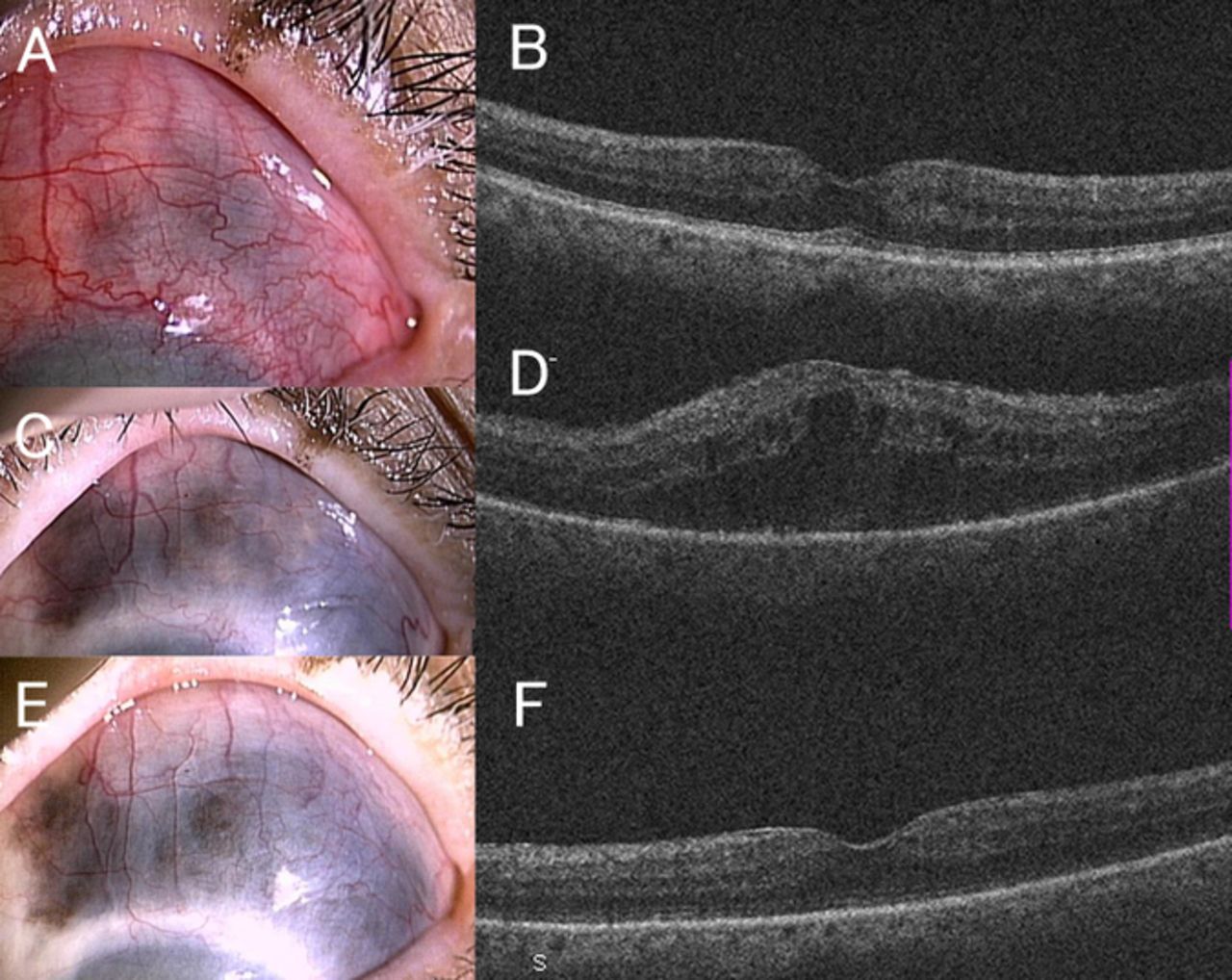
Patient 2. A 50-year-old woman with RA presented with unilateral anterior and posterior scleritis (figure 2A, B). Her visual acuity was 0.8 in the left eye with normal intraocular pressure. Posterior scleritis was improved with prednisolone, cyclosporine and methotrexate (MTX); however, anterior scleritis was resistant to these treatments. Therefore, infliximab infusions (5 mg/kg) were administered every 8 weeks. A good response to anterior scleritis was observed. However, 5 months after starting infliximab, while anterior scleritis remained asymptomatic (figure 2C), posterior scleritis was exacerbated with severe intraocular inflammation and dense vitritis. Her visual acuity decreased to 0.02. Optical coherence tomography images could not be obtained due to the dense vitritis, and B-mode ultrasonography revealed serous retinal detachment (figure 2D). Infliximab was discontinued. The prednisolone dose was increased up to 40 mg, and she restarted cyclosporine therapy. To date, no flare-up of anterior and posterior scleritis has been noted for 12 months (figure 2E, F).
Initial findings of slit-lamp examination and optical coherence tomography in patient 2 with rheumatoid arthritis showing severe anterior and posterior scleritis (A, B). Five months after starting infliximab, slit-lamp examination reveals no anterior scleral hyperaemia (C); however, B-mode ultrasonography reveals dense vitritis and serous retinal detachment (*) (D). After stopping infliximab and restarting steroid and immunosuppressive therapy, both anterior and posterior ocular inflammations were completely resolved (E, F).
Patient 3. A 14-year-old girl was suffering from bilateral chronic anterior uveitis associated with juvenile idiopathic arthritis (JIA). Although joint disease was silent, her ocular disease, diagnosed 6 years previously, was resistant to conventional treatment with prednisolone, cyclosporine and MTX. Her visual acuity was 1.5 in the right eye and 1.0 in the left eye with normal intraocular pressure. Anterior uveitis in her right eye was mild. However, anterior ocular inflammation was severe, and long-term ocular complications, including band-shaped keratopathy, posterior synechia and cataracts, developed in her left eye (figure 3A). Therefore, infliximab infusions (5 mg/kg) were administered every 8 weeks, and bilateral anterior uveitis was ameliorated. Unexpectedly, 10 months after starting infliximab, she experienced exacerbation of severe anterior uveitis in both eyes and developed macular oedema in the right eye (figure 3B). She was treated with sub-Tenon’s capsule triamcinolone acetonide injection to right eye without success. We decided to switch from infliximab to adalimumab. After starting adalimumab, both ocular anterior inflammation and the macular oedema were completely in remission (figure 3C). To date, no flare-up of anterior and posterior uveitis has been noted for 2 years.
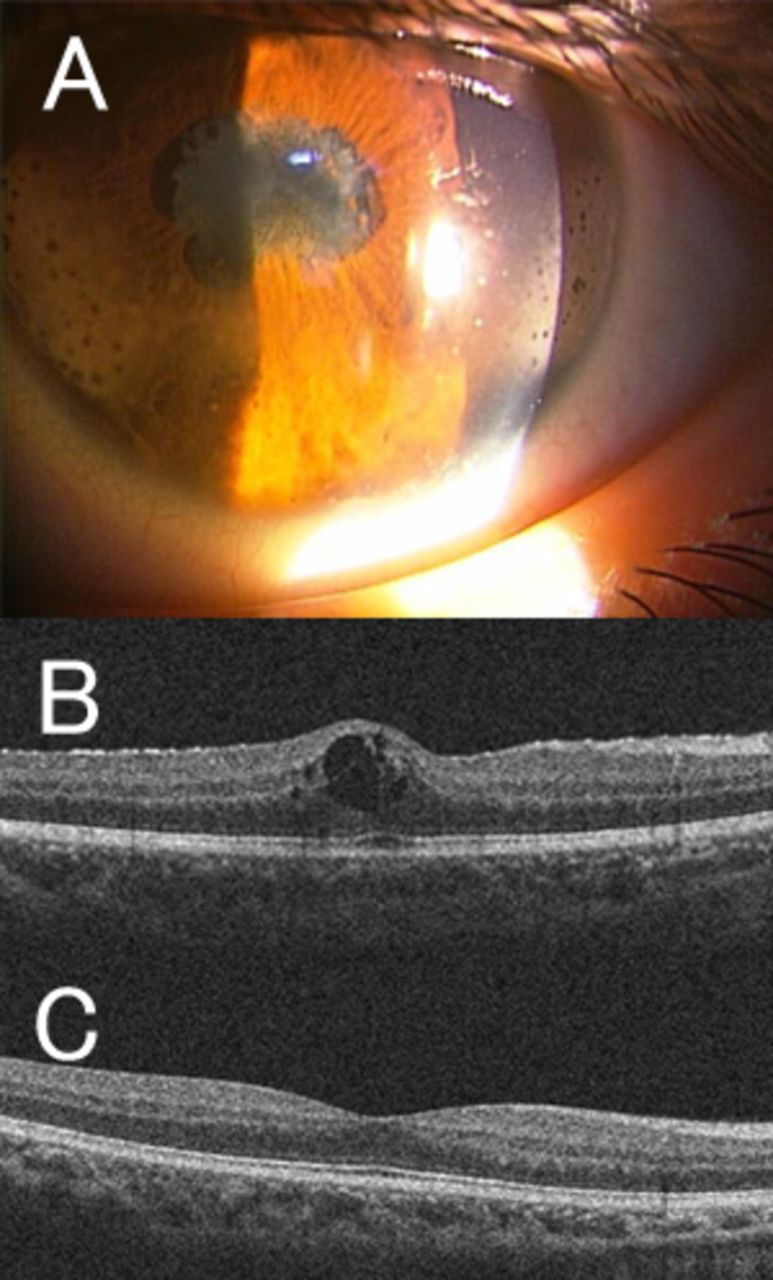
Slit-lamp examination of the left eye in patient 3 with juvenile idiopathic arthritis reveals band-shaped keratopathy, posterior synechia and cataracts (A). Ten months after starting infliximab, optical coherence tomography of the right eye reveals cystoid macular oedema (B). Cystoid macular oedema was resolved after switching to adalimumab (C).
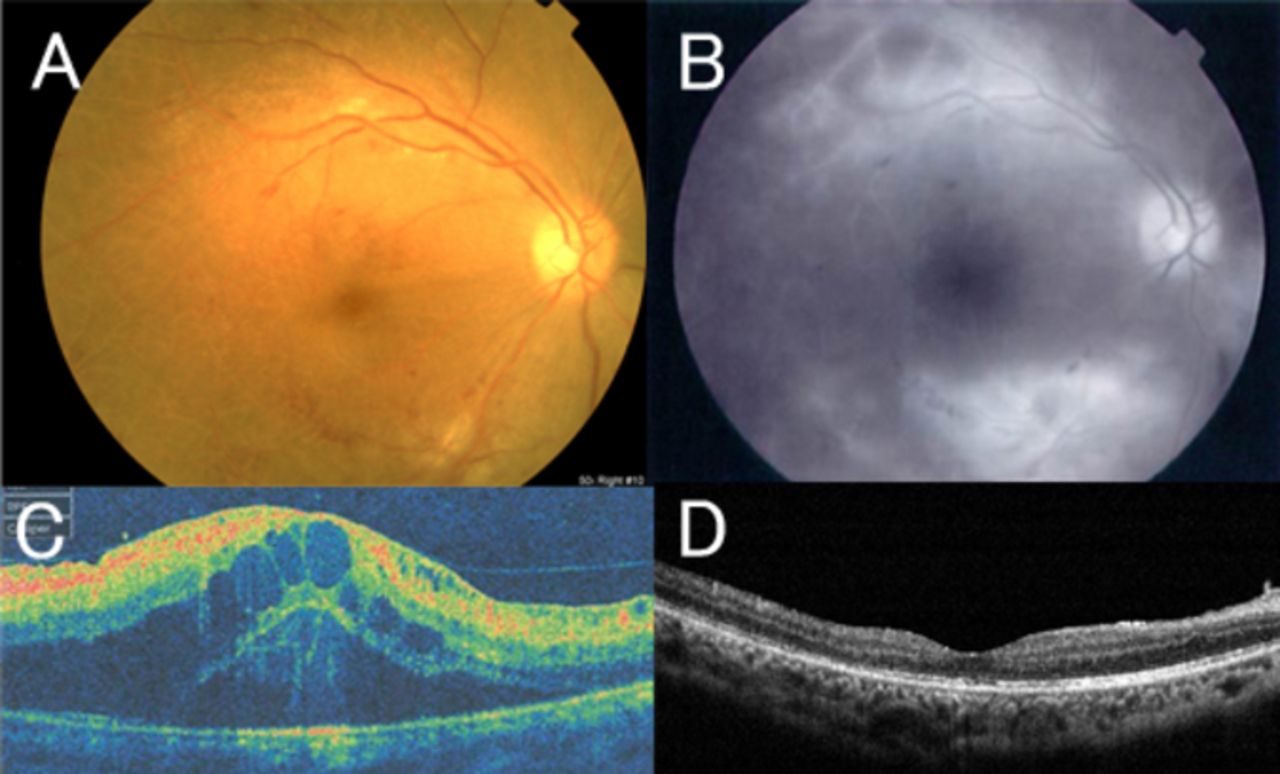
Patient 4. A 17-year-old boy with Crohn’s disease was treated with infliximab infusions (5 mg/kg) for 2 years with subsequent resolution of intestinal symptoms. He presented with blurred vision in the right eye. His visual acuity was 0.05 in the right eye and 1.0 in the left eye with normal intraocular pressure. Dilated fundus examination and fluorescein angiography revealed severe bilateral retinal vasculitis and macular oedema (figure 4A–C). After receiving intravitreal triamcinolone injection, infliximab was switched to adalimumab. Six months after intravitreal triamcinolone injection, macular oedema was improved in both eyes (figure 4D); however, severe retinal pigment epithelial atrophy developed in both eyes. To date, there has been no flare-up of vasculitis for 5 years.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
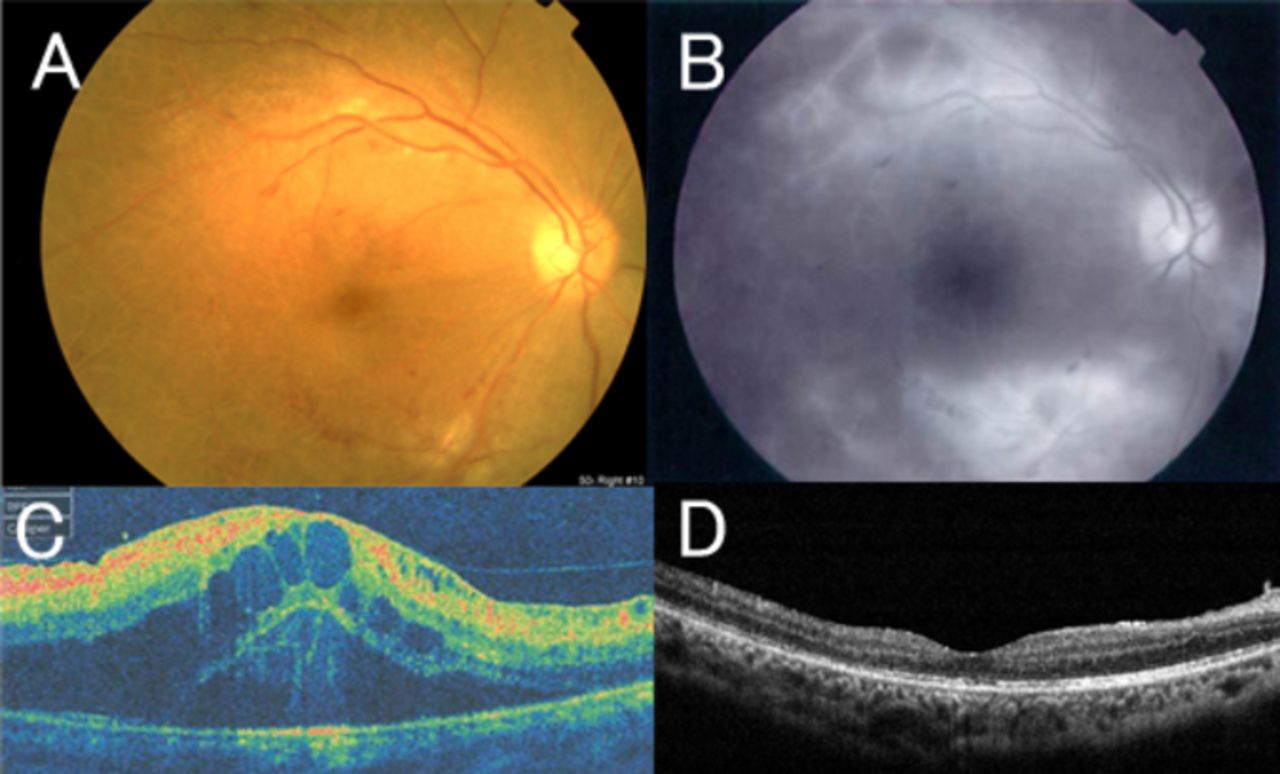
Fundus photograph of patient 4 with Crohn’s disease demonstrating focal sheathing and retinal infiltrates (A). Fluorescein angiography reveals extensive leakage from retinal vessels (B). Optical coherence tomography of the right eye reveals cystoid macular oedema (C). Cystoid macular oedema was resolved after receiving intravitreal triamcinolone injection and switching to adalimumab (D).
Discussion
PAE is defined as the occurrence of a pathological condition that typically responds to a biological agent during therapy with this class of drug. PAEs were mainly described with anti-TNF drugs and more rarely with the other biological classes. Psoriasis and psoriasiform lesions, inflammatory bowel diseases, sarcoidosis, vasculitis and inflammatory eye disease have been described as PAEs of anti-TNF drugs.6–8 TNF-α is one of the key proinflammatory cytokines in non-infectious uveitis. Anti-TNF-α drugs cause programmed cell death of TNF-α expressing activated T lymphocytes and reduces acute phase inflammatory response and decreases both local and systemic levels of inflammatory mediators. However, despite the use of anti-TNF-α agents, there are still some patients with non-infectious uveitis refractory to anti-TNF-α agents.15 This could be the consequence of the existence of TNF-α independent inflammatory pathways in addition to TNF-α dependent pathways. The TNF-α independent inflammatory reactions under anti TNF-α agents may relate to occurrence of PAEs.
Paradoxical ophthalmological manifestations are mainly observed with etanercept. Using a US database of spontaneous reports, Lim et al 9 described 43 cases of new onset of uveitis with etanercept treatment, 14 with infliximab and 2 with adalimumab, and concluded that etanercept is associated with an increased number of uveitis cases compared with infliximab or adalimumab after adjusting for the number of patients treated with each agent. In a French national survey, Wendling et al 10 described 31 cases of new onset of uveitis, including 23 cases with etanercept treatment, 5 with infliximab and 3 with adalimumab.
Paradoxical ophthalmological manifestations are thus observed more often with etanercept and less frequently with infliximab. Only 22 cases of new-onset uveitis with infliximab treatment were reported. From the US database of spontaneous reports, Lim et al 9 reported 14 cases of new-onset uveitis with infliximab treatment. In the French national survey, five cases of new-onset uveitis with infliximab were reported.10 However, details of ocular clinical features were not clearly described in these two reports. Only three case reports have described the details of PAEs under infliximab treatment. Coates et al 12 reported one case of new-onset bilateral uveitis in a patient with RA treated with infliximab, and the condition resolved after infliximab cessation. Singla et al 13 reported another case of new-onset bilateral anterior uveitis in a patient with ulcerative colitis undergoing infliximab treatment, and the condition resolved with steroid eye-drops. Ben Abdelghani et al 14 reported another case of new onset of bilateral occlusive retinal vasculitis with neovascularisation associated with infliximab in a patient with Crohn’s disease-related spondyloarthritis that resolved after laser photocoagulation treatment and peribulbar corticosteroid injection. We described here the details of four cases of new-onset posterior ocular inflammation following administration of infliximab.
Scleritis is a destructive eye disease, and infliximab may be considered in the treatment of non-infectious scleritis refractory to other treatment. de Fidelix et al 16 reviewed 47 cases with scleritis who were treated with infliximab. Forty-five patients (96%) treated for scleritis exhibited ocular benefits, and only three patients had adverse effects, including herpes zoster, allergic reaction and lupus-like reactions. In our cases, infliximab was also effective for anterior scleritis; however, the development of macular oedema, vitritis and intraocular inflammation occurred following infliximab treatment in patients 1 and 2. Infliximab is also reportedly effective in the treatment of refractory cystoid macular oedema-associated non-infectious uveitis;17 therefore, new onset or exacerbation of posterior inflammation observed in these cases was considered to be a paradoxical effect of infliximab. Discontinuation of infliximab and switching from infliximab to tocilizumab (patient 1) or systemic corticosteroid therapy (patient 2) was effective in controlling both scleritis and intraocular inflammation. These results suggest that factors that are not suppressed under infliximab treatment exacerbate intraocular inflammation, which are inhibited by tocilizumab or corticosteroids. Th17 cell expansion under infliximab-stimulated conditions was reported in infliximab non-responder patients with RA.18 Similarly, increased Th17 lymphocyte levels might be related to the development of intraocular inflammation. Corticosteroids affect the distribution and maturation of lymphocytes in the thymus, and tocilizumab inhibits Th17 differentiation.19 The suppression of Th17 cells by tocilizumab or corticosteroids may improve intraocular inflammation in patients 1 and 2.
Ocular involvement is the most severe extra-articular manifestation in patients with JIA. JIA-associated uveitis may lead to structural ocular tissue damage and subsequent visual loss. According to a recent expert panel report on the use of anti-TNF drugs in JIA-associated uveitis, infliximab or adalimumab, rather than etanercept, should be considered as second-line immunomodulatory treatments after MTX.20 However, in patient 3, anterior ocular inflammation was refractory to infliximab, and sight-threatening macular oedema occurred following infliximab treatment, which was considered a PAE. Exacerbated ocular inflammation under infliximab treatment for JIA-associated uveitis has rarely been described. Tynjala et al 21 reported five cases who developed uveitis for the first time while taking anti-TNF treatment for JIA-associated uveitis, four taking etanercept and one taking infliximab. One patient received low-dose (2.4 mg/kg) infliximab treatment, and ocular inflammation resolved after the dose was doubled. An insufficient dose of infliximab may cause uveitis in this case rather than causing a paradoxical effect. In patient 3, macular oedema was observed in JIA-associated uveitis, and distinguishing ocular inflammation related to infliximab inefficacy from that related to a PAE of infliximab is very difficult. Switching TNF inhibitors from infliximab to adalimumab effectively controlled ocular inflammation in this case. Adalimumab is reported to be more efficacious than infliximab in maintaining remission of chronic childhood uveitis including JIA.22 The differences in these agents might be related to the treatment outcome in patient 3; however, the mechanism remains unclear.
The effects of infliximab in the treatment of vasculitis, especially vasculitis associated with RA or Behcet’s disease, have been reported.23 In patient 4, paradoxically, new severe retinal vasculitis was observed under infliximab treatment. Ben Abdelghani et al 14 also reported new onset of occlusive retinal vasculitis with neovascularisation occurring under infliximab in patients with Crohn’s disease related to spondyloarthritis. Neovascularisation associated with intravitreal haemorrhages was observed in this case, and laser photocoagulation sessions and peribulbar corticosteroid injection achieved rapid improvement. In patient 4, laser photocoagulation was not applied because of non-ischaemic retinal vasculitis, and intravitreal triamcinolone injection was performed to control inflammation. However, diffuse retinal pigment epithelial atrophy developed in both eyes as a result of severe vasculitis.
The time range since being on infliximab over development of ocular PAEs was depending on the case. Five patients reported by Wendling et al developed ocular PAEs 10–35 months after starting infliximab.10 In this study, ocular PAEs occurred 4–24 months after starting infliximab. The mechanism of PAEs was unclear, however, PAE might occur in dose-independent manner following administration of infliximab. TNF inhibitors have been used in approximately 2 million patients; however, the number of cases of PAEs following TNF inhibitors was low, implying a genetic predisposition. van Baarsen examined 1623 pharmacogenomic response genes affected by infliximab and reported interindividual difference in the magnitude of pharmacological response to infliximab.24
Hypotheses regarding imbalances in the cytokine milieu have been proposed for psoriasis, which is the most common PAE, as well as a shift towards a Th1 cytokine profile or production of interferon-α (IFNα).25 TNF downregulates the production of IFNs by plasmacytoid dendritic cells. Thus, inhibiting TNF enhances IFN production and favours psoriasis development. Another mechanism may involve increased expression of chemokines and receptors induced by IFNα, leading to increased homing of lymphocytes in the skin. Similarly, in paradoxical ocular inflammation, increased IFN expression and homing of Th1 cells to the uvea may induce new-onset uveitis. Further research and investigation are necessary to gain a clearer understanding of PAEs and explain differences in the incidence rates among TNF inhibitors.
We described here four cases of new onset or exacerbation of uveitis following administration of infliximab. All cases developed or exhibited exacerbated posterior ocular inflammation. Three patients developed macular oedema, and exacerbation of intraocular inflammation with vitritis developed in another patient. Three of four patients were taking infliximab for coexistent ocular disease. Ocular inflammation is paradoxically a potential adverse effect of infliximab even if it is administered for the treatment of ocular inflammation. Therefore, paradoxical ocular inflammation and risk of infections should be considered during a course of TNF inhibitors. However, this study had some limitations, including its observational nature, the small number of cases and the difficulty of distinguishing ocular inflammation related to underlying disease from PAEs. Ocular inflammation is paradoxically a potential adverse effect of infliximab. Patients being treated with infliximab should be closely monitored for the development of new ocular inflammations.
Acknowledgments
Language editing assistance: Enago for the English language review.
References
Footnotes
Contributors CI researched the ophthalmological data and wrote the manuscript. HO, MH, TM and HS performed the ophthalmological examinations and reviewed the manuscript. HM and NO supervised the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This research was approved by the Institutional Review Board of JCHO Osaka Hospital (No 2017-30).
Provenance and peer review Not commissioned; externally peer reviewed.