Article Text

Abstract
Objective Blue light hazards for retina and ocular surface have been repeatedly described and many protective methods are introduced for retina; however, no study has been conducted on ocular surface protection. The purpose of this in vitro study was to examine phototoxicity and shade protection after blue light irradiation in primary human cells of corneal surface origin.
Methods and analysis Primary human cells of corneal surface origin were obtained from eye bank eyes. After blue light irradiation (405 nm) of these cells for 3 min, and a further 24 hours’ incubation, surviving viable cells were assessed by the methyl thiazolyl tetrazolium assay. Simultaneously, cell viability was determined in wells covered by ultraviolet and blue light shades.
Results Under subconfluent conditions, viable cells decreased by around 50% after blue light irradiation, compared with control cells without irradiation. The blue light phototoxicity was not blocked by the control shade, but the ultraviolet-blocking and blue light-blocking shades protected the cells from phototoxicity, producing a 30%–40% reduction (ultraviolet) and 15%–30% reduction (blue light) in viable cells.
Conclusion These results indicate that blue light injures ocular surface cells and the cells are protected from damage by a shade. We recommend blue light protection to maintain ocular health, especially in high-risk populations, such as people with dry eye, contact lens users, the malnourished and the elderly.
- cornea
- conjunctiva
- ocular surface
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Cell culture studies have described blue light as harmful to ocular surface cells in a dose-dependent manner. However, the protective effect of light-blocking shades has not yet been examined.
What are the new findings?
Our results demonstrate the phototoxicity of blue light for established primary cultures of human corneal surface cells. Ultraviolet-blocking and blue light-blocking shades are effective in protecting the cells from blue light-induced damage.
How might these results change the focus of research or clinical practice?
Blue light may cause potential damage to ocular health and protective measures are recommended, especially in high-risk populations, such as people with dry eye, contact lens users, the malnourished and the elderly.
Introduction
The term ‘light pollution’ as a human health-related environmental problem is well known, as light environments have grown at night and have become potentially harmful to health.1 2 Improper exposure to artificially emitted blue light (visible light with a wavelength of 400–500 nm) at night has several disadvantages, such as circadian rhythm disorders, sleep disorders, mood disorders, carcinogenesis and many other health problems.2–5 Additionally, blue light may affect vision and the ocular surface.6–11
Phototoxicity of blue light against retinal cells has been documented for decades12 and experimental results have repeatedly indicated its harmfulness to retinal pigment epithelium and photoreceptor cells.13–19 Since the pathophysiology of experimental retinal damage resembles age-related macular degeneration, a serious vision-threatening disease in elderly people,20 the effects of light shields and intraocular lenses have been evaluated for the purpose of prevention of age-related macular degeneration,13–17 although clinical evidence is still lacking.21 Numerous investigations have been conducted on ocular surface cells looking at the effects of ultraviolet (UV) radiation and protection for the cornea and conjunctiva.22–26 In contrast, only four studies8–11 have described phototoxicity and increased oxidative stress in ocular surface tissue and cells irradiated with blue light. One study11 suggested the clinical implication that blue light may induce oxidative damage in the ocular surface of patients with dry eye disease (DED). Potential protection of the ocular surface from blue light hazards includes eyewear shields, blocking shades, blue light emission control software and extracts of medicinal plants.27–29 However, no study has been conducted on ocular surface protection by light-blocking shades.
The purpose of this study was to examine the phototoxicity after blue light irradiation of human ocular surface cells. In addition, we examined the protective effect of light-blocking shades on blue light phototoxicity of ocular cells. We previously reported phototoxicity of blue light in commercially available cultured corneoconjunctival cells.8 In the present study, we established primary cell culture experiments with human ocular surface cells, and examined the phototoxicity of blue light in relation to protection with light-blocking shades.
Materials and methods
Primary culture of human ocular cells
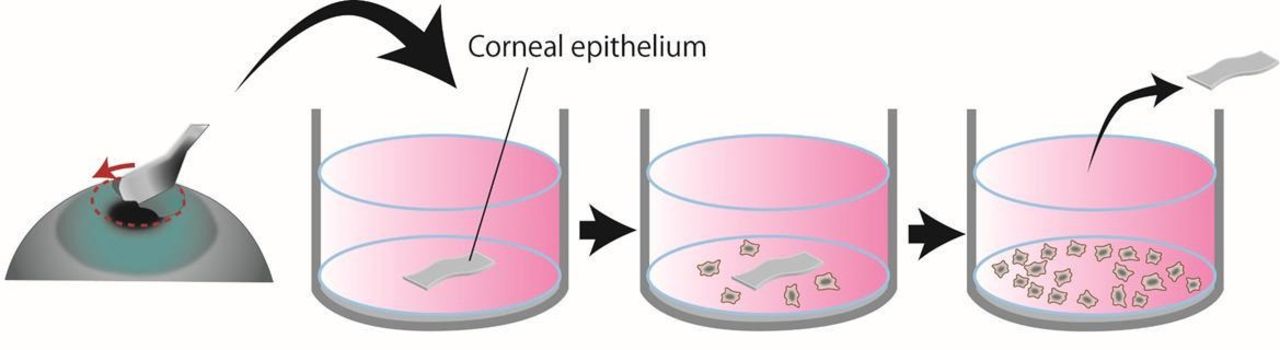
One human eye was supplied from SightLife (Seattle, WA, USA). According to the supplier, the human eyes was preserved in a corneal storage medium Optisol (Chiron Ophthalmics, Irvine, CA, USA) and dissection of eyeball was performed within 5 days after enucleation. Corneal epithelium was carefully peeled off from the eyeball and incubated in Dulbecco’s Modified Eagle Medium (DMEM, Thermo Fisher Scientific, Waltham, MA, USA) containing 15% fetal bovine serum (FBS, Thermo Fisher Scientific), 2 ng/mL recombinant human basic fibroblast growth factor (bFGF, Thermo Fisher Scientific), 30 mg/L L-glutamine (Thermo Fisher Scientific), 2.5 mg/L Fungizone (Thermo Fisher Scientific) and 2.5 mg/L doxycycline (Thermo Fisher Scientific) at 37℃ in humidified 5% CO2. Outgrown cells (cells of corneal surface origin, CsCSO) were cultured in the same medium and the medium was exchanged every 3 days. Figure 1 shows a schematic figure for this process. After cell numbers reached sufficient levels for assay after approximately 2 weeks of culture, cells were harvested and stored at −80℃ until assayed.

Schematic illustration for the process of getting human cells from corneal surface. Corneal epithelium was carefully peeled off from the eyeball using surgical knife and incubated in culture medium. Outgrown cells were cultured in the same medium and the medium was changed every 3 days. After cell numbers reached sufficient levels for assay in approximately 2 weeks of culture, cells were harvested and stored at −80°C until assayed.
Immunohistochemical staining for keratin with anti-pan-keratin antibody
DMEM containing 15% FBS, 2 ng/mL bFGF, 100 U/mL penicillin (Wako Pure Chemicals, Osaka, Japan) and 0.1 mg/mL streptomycin (Wako Pure Chemicals) was used as a medium. Normal human dermal fibroblasts (NHDF, DS Pharma Biomedical, Osaka, Japan) were used as a negative control. An aliquot (0.5 mL) of the medium containing approximately 2×104 cells (CsCSO or NHDFs) was seeded to each well of a 24-well culture plate and incubated at 37 ℃ in humidified 5% CO2 for 2 weeks for confluent condition. Then the cells were fixed in cold methanol for 10 min followed by washing twice with phosphate buffered saline (PBS, pH 7.4). After blocking with a solution consisting of 10% normal donkey serum (Calbiochem, San Diego, USA) and 0.1% Triton-X in PBS, the cells were incubated with anti-pan-keratin antibody (2 µg/mL, mouse anti-keratin type I+II, clone AE1/AE3, mouse IgG1, No 61835, Progen, Heidelberg, Germany) for 60 min at room temperature. Next, the cells were washed three times with PBS and were incubated with Alexa flour 488-conjugated donkey anti-mouse IgG (1 µg/mL, A21202, Thermo Fisher Scientific) for 30 min at room temperature. For isotype controls, mouse IgG1 (0.2 µg/mL, clone MOPC21, M5284, lot 026K4804, Sigma-Aldrich) was used instead of anti-pan-keratin antibody. Nuclei were stained with 1 µg/mL of 4,6-diamidino-2-phenylindole (Dojindo Laboratories, Kamamoto, Japan). Finally, the cells were analysed using a fluorescent microscope (Axio Observer, Carl Zeiss, Oberkochen, Germany).
Light-blocking shades
Three kinds of shades were used. The spectrum transmittance of each shade measured by a spectrophotometer (UV-2600; Shimadzu, Kyoto, Japan) in our previous study14 is shown in figure 2. These specifications were measured according to EN ISO 12312-1:2013. The control shade made of acrylic polymers (termed control shield hereafter, Acrylite; Mitsubishi Rayon, Tokyo, Japan) allows the passage of almost all optical wavelengths of light (figure 2A). The violet-blocking shade made of NXT clear UV (JINSClear; IC-Japan, Tokyo, Japan) completely blocks UV light and blocks partially visible light around 400–450 nm (figure 2B). The blue-plus-blocking shade made of NXT HCD 554/80 (JINSPC brown; IC-Japan) completely blocks UV light and blocks visible light around 400–450 nm more efficiently than the violet-blocking shade (figure 2C).

Spectral transmittance of light-blocking shades. (A) Control shade made of acrylic polymers (Acrylite, Mitsubishi Rayon). (B) Violet-blocking shade made of NXT clear UV (JINSClear, IC-Japan). (C) Blue-plus-blocking shade made of NXT HCD 554/80 (JINSPC brown, IC-Japan). Reproduced with permission from Narimatsu T, Ozawa Y, Miyake S, et al 14
Assay method and blue light irradiation for examining phototoxicity
An aliquot (100 µL) of medium containing approximately 2×104 CsCSO was seeded into each well of a 96-well culture plate and incubated at 37℃ in humidified 5% CO2 for 26–28 hours for 20%–40% confluent conditions. Then, the well was irradiated with blue light (405 nm with an irradiance of 930 mW/cm2) for 3 min. The wavelength and irradiance were based on our previous study in which 405 nm with an irradiance of 930 mW/cm2 could exert distinct cytotoxicity on rabbit corneal epithelial cell lines.8 A continuous-wave laser device equipped with a laser diode of indium gallium nitride (RV-1000; Ricoh Optical Industry, Hanamaki, Japan) was used as the blue light source. To examine the photoprotective effect of three kinds of light-blocking shades, each shade was placed on the well during blue light irradiation. The cells were further incubated for 24 hours to determine surviving viable cells by the methyl thiazolyl tetrazolium (MTT) assay,30 31 in which insoluble formazan converted from MTT was colorimetrically quantified at 595 nm using a microplate reader (FilterMax F5; Molecular Devices, Sunnyvale, California, USA). The MTT assay was performed using a kit (TACS MTT Cell Proliferation Assay; Trevigen, Gaithersburg, Maryland, USA). The experiment in each group was performed on four independent occasions with a single well and two spectroscopic measurements per each treatment as technical repeats. Data processing was carried out as follows: (1) the mean value was calculated from the optical density values in the control group in the MTT assay; (2) the mean value of the control group was set as 100%; and (3) each optical density value in all the groups was converted to % of the mean value (100%) of the control group. As such, the experimental unit (expressed as MTT value) was defined as % of the mean value (100%) of the control group. Since MTT assays assess mitochondrial activity in viable cells,30 31 there always remains a possibility that cell viability is not correctly assessed under certain conditions. Thus, the cells were microscopically checked after adding MTT reagent as shown in online supplementary figure S1.
Supplemental material
Statistical analysis
Two-way analysis of variance (ANOVA) was performed to determine if shade treatment significantly affected the viable cells. P<0.05 was considered significant.
Patient and public involvement statement
Patients were not involved.
Results
Representative immunofluorescence microscopy images of cultured cells and NHDFs for pan keratin immunoreactivity are shown in figure 3. Keratin was detected in some cultured cells but not in NHDFs, and fibroblast-like cells found in cultured cells were keratin negative. Thus, the cultured cells were regarded as a mixture of keratinocyte and fibroblast-like cells. Using the cultured cells, the photoprotective effect of three kinds of shades as well as the phototoxic effect of blue light irradiation for 3 min was compared (figure 4). MTT values of tested cells from central and peripheral corneal portion decreased similarly by around 50% after blue light irradiation compared with corresponding control MTT values without blue light irradiation. The phototoxicity caused by blue light was not blocked by the control shade, while the violet-blocking shade and the blue-plus-blocking shade protected the cells from the phototoxicity to a greater or lesser extent. The violet-blocking shade resulted in an approximate 30%–40% reduction in viable cells of both populations, while the blue-plus-blocking shade resulted in around a 15%–30% reduction. Indeed, the two-way ANOVA showed a significant shade treatment effect on the number of viable cells. The photoprotective effect of the violet-blocking shade was compared with the blue-plus-blocking shade, and the latter was apparently superior to the former.

Representative fluorescent microscopic images of immunostained cells with anti-pan-keratin antibody and its isotype control antibody (mouse IgG1). (A, B) Cells from human corneal surface origin (peripheral portion) and normal human dermal fibroblasts immunostained with anti-pan-keratin antibody, respectively. (C, D) Cells from human corneal surface origin (peripheral portion) and normal human dermal fibroblasts immunostained with an isotype control antibody (mouse IgG1), respectively. Scale bar=100 µm.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The photoprotective effect of various light-blocking shades on viable cells assessed by the methyl thiazolyl tetrazolium (MTT) assay in corneal surface cells (central and peripheral portion) 24 hours after blue light irradiation at 405 nm with irradiance of 930 mW/cm2 for 3 min. The mean optical density value in each control group was set as 100%, and all the optical density values in the corresponding experimental groups were converted to % of the mean (100%) of each control group. As such, the experimental unit is expressed as MTT value. Each column represents the mean with individual data (black dots) that were obtained from each independent assay. ANOVA, analysis of variance.
Discussion
The present study suggests that blue light may be toxic for human ocular surface cells, as demonstrated by the in vitro culture study in which the toxic effect of blue light was alleviated to a greater or lesser extent by shades that blocked light around 400–450 nm. When the blue-plus-blocking shade was used, it attenuated the toxic effect more prominently than did the violet-blocking shade. Since the blue-plus-blocking shade blocks visible blue light around 400–450 nm more effectively than the violet-blocking shade, it is strongly suggestive of blue light being a toxic agent to ocular cells. This study is the first to investigate the protective effect of light-blocking shades against blue light phototoxicity in human ocular surface cells, and these results are consistent with previous investigations with retinal cells.13 14
Ant-pan keratin antibody used in the present study was immunoreactive with AE1/A3 that is a group of keratin filaments with both low and high molecular weights, and the keratin is expressed in epithelial cells.32 However, the microscopic images showed that fibroblast-like cells found in cultured cells were keratin negative. Regarding the reason why keratin was not detected in all the cultured cells, it is considered that bFGF in the culture medium mediated epithelial mesenchymal transformation (EMT) as reviewed by Lee et al.33 It was reported that adult human corneal epithelial cells (HCEC) are mitotically inactive and are arrested at the G1 phase of the cell cycle.34 However, when cornea is injured, HCECs could resume proliferation and alter their cell morphology known as EMT, and in vitro studies revealed that EMT is mediated by bFGF.35 36 As such, it is suggested that bFGF supplemented in the medium induced EMT in the present study. In addition to EMT, contamination of fibroblasts derived from corneal keratocytes may need to be considered. Corneal keratocytes residing in stroma are quiescent cells. Once injury or infection occurs, these cells lose their quiescent state and acquire activated phenotypes that have the properties of fibroblasts and myofibroblasts.37–39 It was reported that keratocytes can be activated in vitro by growth factors such as transforming growth factor-β, platelet-derived growth factor and bFGF.40–42 Accordingly, a possibility that some corneal keratocytes contaminated in the cell culture proliferated in the presence of bFGF could not be excluded in the present study.
Even under the in vitro conditions where some tested cells exhibited fibroblastic feature and they were regarded as a mixed population of keratinocyte and fibroblast-like cells, the present study suggests that blue light may be toxic for human ocular surface cells, as demonstrated by the in vitro culture study in which the toxic effect of blue light was alleviated to a greater or lesser extent by shades that blocked light around 400–450 nm.
Regarding the underlying mechanism by which blue light induces a toxic effect on ocular cells, reactive oxygen species (ROS) has been suggested to be involved.9–11 That is, exposure to blue light provokes ROS overproduction via mitochondrial damage. Since it was reported that the absorption spectrum of a whole mitochondrial suspension in a reduced state gives a peak between 400 and 450 nm,43 405 nm blue light could be absorbed by mitochondria. Thus, to confirm the involvement of ROS, the ameliorating effect of ROS-specific scavengers on the phototoxic effect should be examined following identification of ROS in the near future.
We speculate that long-term exposure to blue light from portable devices emitting blue light from a short distance may cause potential damage to ocular health, especially in high-risk populations,11 44 such as people with DED, contact lens users, the malnourished and the elderly, due to accumulated oxidative stress that is a result of an imbalance between ROS generation and scavenging.
Oxidative stress evoked by blue light exacerbates DED as suggested in previous investigations.45–48 This could become a common health problem since office workers in modern society are at risk of DED.49 In addition, blue light could aggravate the DED-related visual symptoms, such as blurred retinal images caused by increased scattering at the ocular surface due to an unstable tear film.6 7 Additionally, patients with DED may have dermatologic (eg, rosacea, scleroderma)50 and systemic problems (eg, rheumatological diseases) that are not yet diagnosed. Some of them may have light sensitivity and need to be careful of light exposure. Besides DED and its related symptoms, there are a number of unsolved issues related to artificial blue light-induced cellular damage associated with the ocular surface and macula.5 The sunlight spectrum is a uniformly distributed wavelength and its energy is simply dose dependent. By contrast, the modern lighting environment is rapidly changing, and it is made up of different artificial instruments producing a spectral imbalance. Although no report has documented chronic ocular damage from ambient fluorescent or incandescent light, we propose that photoprotective measures from ambient lighting conditions should be established.
The limitations of the present study are summarised below. EMT was induced probably by bFGF in the present study, indicating that effects on untransformed HCECs were not completely evaluated. In addition, this is an in vitro cell culture study and should be further confirmed with clinical or animal studies. Only acute phototoxicity was examined in the present study and a long-term study may be better to evaluate tissue damage after accumulated toxicity. Various other light spectra should also be examined, including green, yellow and red lights as these are included in the daily environment.
In conclusion, the present results indicate that blue light injures human ocular surface cells and the cells are protected from damage by a shade. Blue light protection may be recommended for high-risk populations.
Acknowledgments
We are grateful to Dr Yoko Ozawa for providing the experimental shields and Dr Hideyuki Miyashita for technical and scientific contributions.
References
Footnotes
Contributors YN conducted and reported the study. AI, MA and KT were involved in the design and conduct of the study. YN and MA designed the study. YN, MA, KN and KT reviewed the final version of the manuscript. YN, MA and KN are the guarantors.
Funding The study was supported by a JSPS KAKENHI Grant-in-Aid for Scientific Research (C), 17K07788, 2017.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.